The DETAILS BLOG
Capturing Stories from the Field: Reflections, Challenges, & Best Practices

|
By Anna Morgan-Barsamian, MPH, RN, PMP, Senior Manager, Training & Education, NaRCAD An interview with Adriane Apicelli, MSW, Project Manager, Harm Reduction Projects, University of New Hampshire, College of Health and Human Services. Tags: Harm Reduction, Detailing Visits, Evidence-Based Medicine  Anna: Hi, Adriane. Harm reduction is deeply meaningful to many individuals – can you share why harm reduction is meaningful to you? Adriane: The core principles of harm reduction, such as self-determination, mutualism, and self-advocacy, resonate with my personal and professional values. I firmly believe that individuals are the experts in their own lives, and it’s essential that people have access to the necessary resources, materials, and support systems to ensure their safety and well-being. Harm reduction also offers a powerful framework that facilitates a shift within communities that moves away from moralization and stigmatization of individuals who use drugs. It’s easy to blame individuals for their behavior, but it’s far more challenging to critically reflect on how systems and decisions put people in those circumstances in the first place. Anna: By embracing harm reduction principles, people within our communities can foster empathy and understanding for those facing challenges with substance use. Everyone deserves the same dignity, respect, and access to necessary resources. Can you tell me about the harm reduction detailing project you’ve been working on in collaboration with the National Association of County and City Health Officials (NACCHO)? Adriane: We’re currently focused on detailing elected officials in the State of New Hampshire, including city counselors, mayors, and senators. The opinions and decisions of elected officials shape the harm reduction service landscape – they make decisions that either enable or constrain available resources. Anna: Recognizing the influential role of elected officials is crucial when working on public health initiatives, including harm reduction. What is the overall goal of your current detailing project?  Adriane: We want to empower elected officials to make informed decisions that increase capacity of harm reduction services based on the needs of their communities. We’re currently encouraging elected officials to establish direct connections with individuals who use drugs so they can integrate the expertise from those with lived and living experience into decision-making processes regarding laws, policies, and resource allocation. Anna: Actively listening to those with lived and living experience helps to better understand how to support specific populations. How did your team decide to focus on encouraging elected officials to directly connect with people who use drugs? Adriane: During the development of our detailing project, we consulted with local syringe service program (SSP) participants and asked them how they think elected officials can better understand substance use and harm reduction. The overwhelming response was for direct communication between individuals who use drugs and elected officials, or having elected officials spend the day with them to understand their experiences firsthand. We’re trying to figure out how we can facilitate these approaches to ensure the safety and ethical treatment of SSP participants. We’ve also been exploring the possibility of forming advisory committees to incorporate the perspectives of individuals who use drugs in the decision-making process in a safe and supportive environment.  Anna: Advisory committees certainly help to ensure that voices and perspectives are heard and valued. Let’s transition to thinking about all of your detailing work to date – what makes you most proud to be a harm reduction detailer? Adriane: The people I detail. We shouldn’t underestimate how hard it is to change our minds, our attitudes, or our behaviors. It takes so much humility and effort to receive and integrate new information, especially when it counters your social values and beliefs. It’s an honor to work through that learning process with those that I detail. Anna: Do you have a specific example of that learning process that you can share? Adriane: I detailed someone who was initially hesitant to publicly announce that she prescribes buprenorphine because she was worried how that information would affect her patient panel. We ended up having a conversation about substance use stigma and its implications. We discussed that openly sharing that she prescribes buprenorphine serves as a powerful signal to patients, assuring them that she provides a safe environment to seek treatment. It also sends a message to other clinicians about the importance of prescribing this medication to patients who need it.  Anna: Having those types of honest conversations with people you detail is imperative to changing behaviors and reducing stigma at the individual and community level. Is there anything else you’d like to add before we wrap up today? Adriane: Remember that it’s much easier to build harm reduction capacity in collaboration with others. Last year, I collaborated with individuals from the public health department, a local hospital, the New Hampshire Harm Reduction Coalition (NHHRC), and a community volunteer to address a concern raised by a business owner regarding improperly discarded sharps on their property. We formed an informal work group and created a proposal aimed at piloting an anonymous syringe disposal project, installing two disposal units in the community. The disposal units were proposed to be on city property, so we needed buy-in from City Council to be able to do this. We recognized the power of engaging elected officials and presented our proposal to the City Council. Our proposal received unanimous support and it’s currently being piloted in the community. Collaborative advocacy and engagement with members of the community and elected officials can bring about positive change and enhance the health of all. Anna: We often have more power than we think when we collaborate with others who have similar goals. Detailing is an effective approach for encouraging collaboration and connection with experts in the community, including experts with lived and living experience. Thanks for joining us today, Adriane! We look forward to continuing to hear about your inspiring harm reduction work in New Hampshire. Have thoughts on our DETAILS Blog posts? You can head on over to our Discussion Forum to continue the conversation!  Biography. Since 2020, Adriane Apicelli has served as the Project Manager and primary academic detailer of the University of New Hampshire (UNH), Department of Nursing’s Harm Reduction Education and Technical Assistance (HRETA) project. She holds a Master of Social Work (MSW) from Boston College, where she also earned a Certificate in Management. In addition to her role with the HRETA project, Adriane serves as a nonprofit strategic planning consultant and has previously served as an adjunct professor for the Department of Social Work at UNH.
By Anna Morgan-Barsamian, MPH, RN, PMP, Senior Manager, Training & Education, NaRCAD An interview with Rocko Cook, Public Health Detailer and Public Health Detailing Program Manager, Detailing Improved Sexual Health (DISH), Arizona State University. Tags: Detailing Visits, Evidence-Based Medicine, HIV/AIDS  Anna: Hi, Rocko – thanks for joining DETAILS today! HIV prevention work is critical and often deeply meaningful to those working in the field. Can you tell me why this work speaks to you? Rocko: I found out I was positive for HIV and syphilis in 2002. I encountered firsthand the stigma and shame associated with these diagnoses. It was devastating, but it’s made me feel even more connected to the work I’m currently involved in. I’ve worked in various roles in the field of HIV prevention and care since 1994, just two years before medication was widely available. In the 90s, there was little support for people who tested positive for HIV from a care perspective, financial perspective, and housing perspective. We now have the medications and tools to prevent, treat, and support people with HIV. Despite this, there’s an urgent need to continue educating clinicians, staff, case managers, community health workers, and other people who are on the frontlines about these tools and resources. Academic detailing helps to close that gap and gives me the opportunity to live my passion of educating others about HIV.  Anna: Thank you for your openness in sharing your personal and professional experiences. Your passion for HIV prevention and care is evident. What’s the number one thing you want clinicians and staff in your community to do differently when it comes to HIV? Rocko: I’d love for them to change the culture of the entire clinic space and create a more welcoming environment for patients. There needs to be a focus on consistent communication coming from every professional a patient meets with when receiving care. All clinicians and staff need to be able to communicate with patients in a sex-positive way and in a way that connects with patients’ specific experiences, identities, and needs. They need to be comfortable communicating about sexual behavior, testing, and PrEP. It’s difficult to have these conversations. I've been doing this for a long time and I’m not perfect at it either, but once we practice and start getting comfortable with ourselves, then it gets a lot easier to be comfortable with patients. Anna: Modeling this type of communication during a detailing visit is key. It can help clinicians and staff feel more comfortable having the same conversations with patients. Can you share a story from the field about a positive response or reaction from someone you detailed? Rocko: There was an agency we worked with that hired a new physician, testers, and medical assistants for their mobile medical and HIV testing unit. They had never worked with this patient population, so our team did several trainings and 1:1 detailing sessions where we role played conversations with patients. We needed to bring them up to speed on how to have gender inclusive conversations and communicate with sex positivity. We had a lot of fun together. The team ended up going to Phoenix Pride to do a big testing event. We were delighted with their success in providing testing to the community and creating a welcoming and safe environment for people interested in being tested.  Anna: That’s a large event for the mobile unit team to tackle, while also succeeding in creating a safe space for all! Let’s talk a little bit more about the impact on patients. Can you share any data on the impact of your detailing work? Rocko: We have anecdotal evidence that folks are benefiting from our services. My colleague and I are closely involved in the gay community and people often tell us about their care experiences. We’re in an enviable position because we know a lot of people and hear things in passing. It helps us do a better job targeting our services; we can work directly with clinics that we’ve heard would benefit from detailing. I also recently connected with someone of trans experience who was tested at Phoenix Pride. They’ve had poor encounters in the past where clinicians and staff assumed the body parts they have. They shared that they had a positive experience with the mobile unit and felt comfortable throughout the visit. Being able to see our impact firsthand has been really motivating for me; it makes my heart sing. Anna: It’s rare to be so closely connected to the community that’s being impacted by your detailing work. It’s clearly been beneficial for your detailing efforts and getting your program up and running. Let’s wrap up with a final question - what has made you most proud of this project so far?  Rocko: I’m so proud of the way our team has come together and engaged with partners across the state. We’ve been able to leverage partnerships and community relationships to enhance program development, implementation, and dissemination. I’m also proud of our creativity in choosing our program’s name, DISH AZ (Detailing Improved Sexual Health). We send out a Weekly Special with a buffet of options on new evidence and information related to HIV prevention and care. We’re creating an active and robust network of professionals, while using food as our motivator! Anna: That’s an innovative way to keep your network engaged! We’re looking forward to hearing about your program as your team continues to expand its network and positively impact more people in the community. Thanks for chatting with us today and sharing your experiences, Rocko! Your passion for this work is palpable. Have thoughts on our DETAILS Blog posts? You can head on over to our Discussion Forum to continue the conversation!  Biography. Rocko Cook serves as the Program Manager for DISH-AZ (Detailing for Improved Sexual Health in Arizona), a program of the Office of Evaluation and Partner Contracts for the Southwest Interdisciplinary Research Center (SIRC) at Arizona State University in partnership with Arizona Department of Health and Human Services. Rocko began working in the field of HIV in 1994 and is a community leader with over 15 years of experience implementing prevention and care programs in Arizona, Ohio, and Kentucky. In addition to his duties as a program manager, Rocko has served as a public speaker, presenter at local and national conferences, and as a consultant and leader for HIV community planning groups. Rocko has been living with HIV since 2002 and is passionate about improving sexual health for all communities.
By Anna Morgan-Barsamian, MPH, RN, PMP, Senior Manager, Training & Education, NaRCAD An interview with Meghan Breckling, PharmD, BCACP, Ambulatory Care Pharmacist and Academic Detailer, University of Arkansas for Medical Sciences and Arkansas Department of Health. Tags: Detailing Visits, Opioid Safety, Harm Reduction, Evidence-Based Medicine 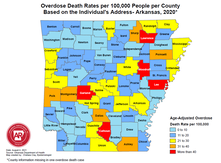 Overdose Deaths Rates per 100,000 people per County, Arkansas 2020 Overdose Deaths Rates per 100,000 people per County, Arkansas 2020 Anna: Hi, Meghan. Thanks for joining me on DETAILS today! Your team has done extensive work on pain management detailing, and you recently completed a pilot project on harm reduction in collaboration with the National Association of County and City Health Officials (NACCHO). Can you tell me a little more about this project? Meghan: Thanks for having me! We decided to target rural counties in Arkansas that have both high drug overdose deaths and naloxone administration rates. We previously created broad pain management materials for our other opioid safety detailing projects; this project took those materials to the next level. We looked at how we could better support clinicians in caring for their patients with substance use disorder (SUD) through a harm reduction lens. We provided clinicians with screening tools to help identify patients with mental health conditions and SUD to determine who could benefit from additional services. We even created a local resource guide for clinicians to easily connect patients to community services. The clinicians found that these accessible tools helped them have open conversations with patients.  Anna: I can imagine having something tangible to give to patients makes clinicians feel more equipped to have these conversations. What other resources were you able to share with clinicians? Meghan: We encouraged clinicians to utilize a new, free mental health resource called AR ConnectNow. This program provides immediate virtual care to all Arkansans dealing with mental health and substance use disorders. Clinicians were grateful for AR ConnectNow because mental health services are scarce in rural Arkansas; they’ve been sharing it with their patients frequently. Anna: You must have been proud to be part of a project that had such an impact on both patients and clinicians. How did the harm reduction lens inform your detailing visits for this project compared to your prior pain management-focused visits? Meghan: Many visits centered on communication with patients. Communication and empathy are two huge pieces to consider with this topic. We spent a lot of time asking clinicians about the conversations they have with patients and the types of questions they ask about substance use. We really wanted to understand what was going well and where there were gaps that we could help fill with resources and support. We also focused on naloxone prescribing and administration. We gave out free naloxone kits to all clinicians that they could either keep in the clinic or give to a patient who was having trouble accessing it. Clinicians were open to the idea of prescribing naloxone to patients who were at risk of overdose and open to keeping kits in their clinic in the event of an overdose. Our team had a lot of clinicians say during follow up visits that they felt more comfortable prescribing naloxone and were prescribing it more to patients and family members.  Anna: It’s impressive how you were able to clearly shift your focus from opioid prescribing to harm reduction and prioritize the relationship between the clinician and patient. Did you receive any pushback from clinicians on harm reduction? Meghan: Clinicians understood the need for harm reduction services but were more inclined to refer patients out rather than providing services within their clinics. For example, we found that a lot of clinicians were resistant to prescribing Medications for Opioid Use Disorder (MOUD), either because they were uncomfortable with the steps to do so, or they were told by leadership that they should not prescribe MOUD at their practice. It can sometimes take an hour or more for patients in rural areas to access specialty services that offer MOUD. We’re looking at future projects where we can utilize pharmacists to increase MOUD prescribing in partnership with primary care providers. For instance, a primary care clinician could diagnose SUD and prescribe MOUD, while a pharmacist could monitor the patient throughout treatment. It would take a lot of burden off the clinicians and could possibly make them less resistant to prescribing it.  Anna: Using pharmacists as an integral part of the care team is an excellent idea – you’ll have to let us know if you receive additional funding for this work! Let’s wrap up with a final question. If another program decided to do a detailing project on harm reduction, what advice would you give them before they went out into the field? Meghan: You need to take a step back and remember that there isn’t going to be instant behavior change among clinicians. For a topic this complex, it’s critical to have follow-up visits and continue to be a resource and support for clinicians. Also, be understanding of clinicians and their experiences. They’re dealing with a lot and it’s not easy to change things all at once. Building a relationship and getting a clinician to commit to just one key message is a huge win. Want to learn more? Read about the harm reduction key messages used for this project and the development of those messages on our previous blog post. Have thoughts on our DETAILS Blog posts? You can head on over to our Discussion Forum to continue the conversation!  Biography. Dr. Meghan Breckling is an Ambulatory Care Pharmacy Specialist at the University of Arkansas for Medical Sciences (UAMS) and is a trained Academic Detailer through the National Resource Center for Academic Detailing (NARCAD) within the Center for Health Services Research (CHSR) at UAMS’ Psychiatric Research Institute (PRI). She previously completed a PGY1 Pharmacy Residency and PGY2 Ambulatory Care Residency at the Central Arkansas Veterans Healthcare System (CAVHS). Currently, she is a part of a multidisciplinary academic detailing team comprised of a pharmacist, physician and physical therapist that provide evidence-based solutions, tools and support for chronic pain management to primary care providers across the state of Arkansas.
By Anna Morgan-Barsamian, MPH, RN, PMP, Senior Manager, Training & Education, NaRCAD An interview with Shuchin Shukla, MD, MPH, Faculty Physician, Mountain Area Health Education Center (MAHEC), NaRCAD Training Facilitator Tags: Harm Reduction, Detailing Visits, Evidence-Based Medicine, Opioid Safety  Anna: Welcome to the DETAILS blog, Shuchin! You wear many hats - you’re an addiction medicine physician, an academic detailer, and an academic detailing trainer. Tell us how you got started with academic detailing. Shuchin: I had an interest in marginalized populations and did my residency in the Bronx in New York City. I was a clinician in HIV care for several years before moving with my family to Western North Carolina. Soon after we moved, I began working at our Area Health Education Center (AHEC) and it was evident that addiction was the primary public health and clinical issue that was causing the most harm in my community. Fast forward a few years and one of my colleagues received a Centers for Disease Control and Prevention (CDC) grant and asked if I could attend a NaRCAD training to learn more about AD. The medical board and one of our pharmacists at the Department of Public Health were very interested in using AD for overdose prevention. We started with a pilot where we detailed 10 clinicians and slowly built our program. We now have multiple AD grants we’re working on, including one on adverse childhood experiences (ACEs) and one on harm reduction.  Anna: We often tell programs to start with a small pilot before growing their programs so that they can identify what went well and where there are opportunities for improvement, especially on new detailing topics like ACEs (e.g., key message adoption, clinician response, etc.). You do a lot of education around substance use disorder and mentioned that your team received a harm reduction grant for AD – what does harm reduction mean to you? Shuchin: The goal is, simply enough, to reduce the level of harm that a person may be facing. Harm reduction means having no expectation of a person's behavior and accepting the reality of what people live and do without judgement. It’s about being open with patients so that they’re more likely to come back for a visit where you can continue to have a conversation with them about getting a little bit healthier. There’s evidence to support harm reduction. The research shows that providing harm reduction services, whether it's naloxone or syringe exchange, reduces harm, but also decreases substance use and helps people engage in substance use care and treatment. Anna: Do you see harm reduction being used with other topics beyond substance use disorder?  Shuchin: There are tons of examples of harm reduction that are built into everything we do. Seatbelts, masks, fire escapes, smoke detectors, vaccines, and the FDA regulatory agency are all forms of harm reduction. As a society, we’ve never looked at substance use through this lens because using drugs is so stigmatized. Anna: I imagine it’s difficult to have detailing visits with clinicians because of the type of stigma associated with it, such as thinking that it’s some sort of moral failing. How have clinicians responded to detailing visits on harm reduction? Shuchin: Most of the teaching about harm reduction is unlearning all the inaccurate information we've been taught. We're taught if you use drugs, you're a bad person and you should be penalized. I remember watching the show Cops growing up and there was always a person of color laid out on a car resisting arrest. Law enforcement would pull out a bag of cocaine from the car and say they’ve saved the community. None of this is right, but I saw that on TV as a middle school kid. It’s easy to generate a lot of negative energy about substance use disorder and substances in general from these shows, and clinicians are part of that thinking too. Asking clinicians to talk to their patients about harm reduction is a lot different than asking them to check their Prescription Drug Monitoring Programs (PDMPs) to ensure that patients aren’t receiving multiple prescriptions for controlled substances. Having a conversation with a patient takes empathy and thoughtfulness, whereas checking a PDMP does not. We’ve found that clinicians who have been the most resistant to harm reduction are those who have family members with substance use disorders. They are often angry, and rightfully so.  Anna: It’s imperative to be empathetic during detailing visits, especially on a topic that affects so many people. Let’s explore harm reduction from a different angle. How do your patients respond when you bring up harm reduction during your clinic visits? Shuchin: These are certainly challenging conversations to have, so you need to start off by letting patients know that they aren’t going to get in trouble for sharing this information and you need to acknowledge the trauma and stigma that surrounds substance use. Patients seem grateful that I approach conversations in a straightforward way that doesn’t stigmatize their use of drugs. I’ve never had a patient be offended or confused about why I was talking to them about harm reduction. Their eyes usually widen when I ask them things like how they use their drugs, how they cook their drugs, or where they get their drugs from. They often say, “I’ve never had a doctor like you.” Anna: You must spend a lot of time building trusting relationships with patients so that you can have these conversations. Shuchin: I do. It also helps that the organization I work for, our county commissioners, and our sheriff are all on board with harm reduction. There’s a lot of focus on Naloxone distribution among members of our community, such as law enforcement, first responders, and other clinicians. Our clinic prescribes a lot of medications for opioid use disorder, specifically buprenorphine, which is also a form of harm reduction. We have peer support specialists who meet patients where they’re at and start the conversation about harm reduction with them before they even have their first visit with me.  Anna: It’s definitely critical to have a community that supports the way you practice, as well your program’s AD messaging. Can you share a final tip for other detailers who are working on harm reduction? Shuchin: Harm reduction is an emotional topic for a lot of people, especially folks who are in frequent contact with people who use drugs, like emergency room clinicians or people with lived experience in their families. With this topic, paying attention to the emotions of the clinician you're detailing and acknowledging those emotions before jumping into your key messages is much more important than any other topic I’ve worked on. Be patient and empathetic – every visit counts toward making a change. Have thoughts on our DETAILS Blog posts? You can head on over to our Discussion Forum to continue the conversation!  Biography. Shuchin Shukla, MD, MPH, was born and raised in New Orleans, Louisiana. He completed medical school and public health school at Tulane University and completed a residency in family medicine at Montefiore Medical Center in the Bronx, New York. He worked in the South Bronx for 5 years following residency, providing primary care for adults and children, as well as for adults living with HIV. He also served as medical director for Montefiore Project INSPIRE, a primary care-based Hepatitis C treatment program. He then moved with his family to Asheville, North Carolina, where he currently serves at Mountain Area Health Education Center (MAHEC) as faculty physician and Clinical Director of Health Integration.
He is an associate clinical professor of medicine in the Department of Family Medicine at the School of Medicine, University of North Carolina in Chapel Hill, and is a Diplomate of the American Board of Preventive Medicine, Board-Certified in Addiction Medicine. Additionally, he is a Robert Wood Johnson Clinical Scholar. He leads on various initiatives and projects around addiction, HIV, Hepatitis C, homelessness, and the criminal justice system. His main experience as a detailer has been focused on improving evidence-based provider interventions related to opioids, pain, and addiction. By Anna Morgan-Barsamian, MPH, RN, PMP, Senior Manager, Training & Education, NaRCAD An interview with Jennifer Carefoot, BSc, Pharm, Academic Detailing Pharmacist, BC Provincial Academic Detailing (PAD) Service. Tags: Conference, COVID-19, Detailing Visits, Evidence-Based Medicine  Anna: Hi, Jen! Thanks for joining us on DETAILS today. Earlier this year, your team developed a detailing campaign in one week for the new COVID-19 treatment, Paxlovid, and presented on your work at our NaRCAD conference. I’m excited to learn more about this campaign. Before we jump in, can you give us some background about your organization? Jen: The British Columbia Provincial Academic Detailing Service (BC PAD) launched in 2008 and provides academic detailing to the province of British Columbia. We have 12 full-time pharmacist detailers for the entire province. The program is publicly funded by the BC Ministry of Health and our topics are chosen based on their relevance to primary care clinicians. Here are some quick facts about our program:
 Anna: Your team connects with many clinicians covering a vast geographical area! Can you walk us through the one-week development of the Paxlovid campaign that you presented on at our conference? Jen: Paxlovid was approved in Canada on January 17, 2022. The Province of BC quickly received doses and urgently needed educational sessions for clinicians in the province for safe and appropriate use of this somewhat complicated medication. The PAD team had the expertise in delivering pharmacotherapy and education through detailing visits; we worked with the Ministry of Health and the COVID Therapeutics Committee (CTC) to quickly develop materials. We were out in the field detailing within a week! Anna: That’s an impressive turnaround time to get your team prepared and out in the field! Were clinicians aware of Paxlovid when your team started detailing on the topic?  Jen: Paxlovid was getting a lot of press in the media at the time- it was the first oral treatment readily available for COVID-19. Clinicians knew they would have to know about this medication since their patients would be asking about it. Anna: New information was coming out every day in the media, which isn’t very common for other detailing topics. How was your team able to stay up to date on the emerging evidence on Paxlovid and continue to keep clinicians up to date? Jen: Our team was able to stay up to date through the excellent communication between our PAD director, Terryn Naumann, the CTC, and the Ministry of Health. We would receive updates via email or video conference daily. We also frequently met internally to share questions, successes, and challenges that we were experiencing in the field. To keep clinicians up to date, we chose to not provide them with the PowerPoint presentation from the detailing visits because the information and evidence was constantly changing. We’ve created 24 versions to date! Instead, we emailed a one-page resource to clinicians after our visits that included links to online resources that were updated in real time.  Anna: That’s one of the benefits of sharing resources virtually – the information can be updated and accessed quickly. If you were told you had to create another campaign in one week, what would you do differently? Jen: That’s a tough question! Would we have liked more detailers? Yes. Do I wish there were 24 more hours in my day? Yes. Would we have liked more clinical trial data? Yes. These are all things that are outside of our control. We did the best we could with the evidence and resources we had. I don’t know if we would do it any other way if we had to do it again under the same circumstances. Anna: What you did worked. Do you have any evaluation data from clinicians that you can share? Jen: Our formal evaluation showed:
 Anna: I’m not surprised by these results! Your team has shown impressive data from myriad detailing campaigns. Before we wrap up, can you tell us how your partnerships and team helped make this campaign successful? Jen: It’s important to partner with others who have expertise in the therapeutic area you’re detailing on. You don’t need to reinvent the wheel with evidence. Pull from data and evidence that other AD programs or reliable organizations have previously put together and be open to the idea that evidence changes. Also, remember that it really does take a team! Everyone brought something critical and unique to the table. Our administration team was instrumental in getting our visits booked and our director was transparent with our team throughout the process. Our team was excited, enthusiastic, and proud to have the opportunity to provide this education to clinicians in our province. Anna: Having a team that is open to a challenge and eager to stay up to date on evidence is so important. It’s not realistic for programs to have to create a campaign in a week, but if they ever find themselves in that situation, we know we can all turn to you and your team for support! Have thoughts on our DETAILS Blog posts? You can head on over to our Discussion Forum to continue the conversation!  Biography. Jen is an academic detailer for the BC Provincial Academic Service since 2016 serving beautiful South Vancouver Island. She is passionate about translating evidence to practice, reducing polypharmacy and shared decision making. In her spare time, she enjoys running, gardening, travelling, and spending time with her family outdoors at the lake.
Tags: Conference, Detailing Visits, Stigma Take a peek at the NaRCAD2022 conference materials on our Conference Hub.  Earlier this month, our team at NaRCAD hosted the 10th annual International Conference on Academic Detailing, “Celebrating 10 Years of Community Engagement.” We hopped on the virtual AD bus and heard from programs from across North America and beyond. This year, the conference featured campaigns focused on menopausal hormone therapy, initiation of antiretroviral treatment (iART), falls prevention, COVID-19, biosimilars, antiracist health care, polypharmacy, and opioids. The theme of community engagement was seen throughout the entire 3-day event, and we’re thankful to everyone who joined from around the world. Check out some of the highlights from our 2022 conference below.  Welcome Addresses:
Field Presentations:
 Breakout Sessions:
Expert Panels:
Special Presentation: “Looking Inward: AD as an Intervention for Antiracist Health Care”:
Real-time Roundtable:
 Thank you for all your engagement and support throughout the last 10 years of NaRCAD annual conferences! We are humbled to see how much the AD community has grown and are excited to be able to feature innovations at our conferences that have informed your work over the years. Our team at NaRCAD will continue to provide space for everyone to come together to share ideas, ask questions, and network. We look forward to seeing you in 2023. -The NaRCAD Team A special thank you to all of our NaRCAD2022 presenters as well as our partners at the Agency for Healthcare Research and Quality! Check out the NaRCAD2022 program book for more information on the presenters. Have thoughts on our DETAILS Blog posts?
You can head on over to our Discussion Forum to continue the conversation! By Anna Morgan-Barsamian, MPH, RN, PMP, Senior Manager, Training & Education, NaRCAD An interview with José Peña Bravo, PhD, Health Educator, Florida Department of Health in Duval County. Tags: Detailing Visits, Evidence-Based Medicine, Opioid Safety, Data  Anna: Hi, José! Thanks for joining us on our DETAILS blog today. Your journey that led you to the academic detailing community is unique – can you share that journey with us? José: Yes! My background is not originally in public health. I’m a biomedical researcher by training, specifically preclinical research using animal models. My dissertation work was on understanding the neurophysiological changes and different brain regions involved in behaviors related to substance use. My intention was to stay in academia and start my own lab, but my plans changed during COVID-19 and the opportunity to work with the public health department in Duval County presented itself. It’s been a learning curve for me to switch my perspective from preclinical research to public health—it’s been an enjoyable journey so far! Anna: I’m sure your biomedical research skills have a positive impact with clinicians during your detailing visits too, especially when clinicians want to discuss the neurobiology of substance use disorder. Speaking of visits, your detailing work is funded through CDC’s Overdose Data to Action (OD2A) grant, which seeks to prevent overdoses. Can you tell us about what the work for this grant looks like in Florida?  José: The OD2A project is a team effort across three CDC-funded jurisdictions in Florida. The health departments share that funding with various community organizations, and we all work toward linking patients with substance use disorder to treatment, mental health care, and care coordination services. Our detailing team is closely connected to organizations and resources within our community, and we share these resources with clinicians during our detailing visits. We also have access to aggregate prescription data from our jurisdiction and are continuing to find ways to present and incorporate this data at our visits with clinicians. We share this data and other resources across our three jurisdictions. Anna: We’ve found that many AD programs have been successful when they are closely connected to community resources. NaRCAD recently hosted a detailing training for OD2A recipients that you attended. What was it like to train with other jurisdictions working on the same project? José: It was helpful to hear from other jurisdictions because they’ve all approached their AD work differently based on the gaps in care in their own communities. I was able to hear from AD programs in rural areas and the specific challenges that their patients face with lack of access to care (long travel times, stigma, etc.). I also enjoyed practicing my detailing skills in a space where I felt comfortable making mistakes. It’s valuable to try things out and see how they’ll go before going out in the field. I learned a lot at the training and am excited to try out some of my new skills at my next visit.  Anna: Hearing from other detailers who are doing this important work with you is so helpful as you continue to think about and grow your own program. What advice would you tell other detailers working on the OD2A project? José: If you’re just starting out, reach out to community partners and get a sense of what patients with substance use disorder are experiencing and the challenges they’re facing before you start detailing clinicians. You’ll better be able to represent what is happening in the community and the resources that exist when you’ve done your research first! Anna: That’s terrific advice – a key piece of being an effective detailer is understanding the patient experience for the clinical topic you’re detailing on. So, what’s next for your work and Duval County? José: We’re currently working with our epidemiology team to collect population-level data and present it concisely. We want to be able to efficiently share this data with clinicians in a way that gets their attention and has them compare it to what they’re experiencing in their clinics to ensure an interactive dialogue during detailing visits. Anna: Using data to tell a story helps clinicians see the impact that they have in preventing overdoses and starts a conversation about organizations and resources that exist within communities for patients with substance use disorder. Thanks for sharing your OD2A work with us, José. We look forward to connecting with you and the other OD2A recipients at our conference in November! Have thoughts on our DETAILS Blog posts? You can head on over to our Discussion Forum to continue the conversation!  Biography. José’s background is in Neuroscience preclinical research with over 10 years of experience in the field. His graduate work focused on the study of rodent models of substance abuse and the neurophysiological changes associated with controlled-substance experience. He has additional experience as an undergraduate and graduate level lecturer in different biomedical research topics. José recently transitioned to a position as health educator as part of the Overdose Data to Action (OD2A) program at the Florida Department of Health in Duval County. His role involves the implementation of the academic detailing program including outreach to clinics, integrating novel data and information to education materials, and keeping track of different metrics associated with outreach and AD sessions.
 Tags: Training, Detailing Visits We are proud to announce that our team at NaRCAD has trained over 1000 people in the techniques of academic detailing. We’ve conducted 60 trainings for detailers working on an amazing range of clinical topics since our first techniques training in 2011. Thank you for growing with us as we’ve expanded from two trainings a year to offering eight trainings in 2022. In honor of reaching this milestone, we’ve compiled testimonials from some of our trainees over the past 11 years. "Just the right amount of didactic, practice, then putting it all together—I'm ready to develop materials & try it.” “I now have the confidence to carry out a successful educational visit!" “The small groups were perfect for interacting, getting to know each other's backgrounds, and made conversations and learning enjoyable." “I came away with refined communication skills and improved clinical knowledge, thanks to the outstanding facilitators.” “This was fantastic! I learned so much and [am] definitely more comfortable with detailing. It was friendly and open to mistakes, and I really appreciated it.” “I walked away with great feedback, knowing my strengths and where I can improve.” “It gave me great insights on the skills I need to be a successful detailer!” “This training provides the opportunity to learn about AD in an interactive way that allows for growth though practice.” We’d like to thank our trainees for committing to improving patient outcomes through clinician education. We’d also like to thank all our past and current NaRCAD facilitators for providing our trainees with the skills needed to be successful and confident detailers. We’re excited to share that we’ve had the pleasure of adding four more training facilitators to our team this year. Welcome to the team, Chirag, Jess, Julia, and Shuchin!  We look forward to continuing to work with all of you. Read more testimonials on our testimonial page or share your training experiences with us below!
-The NaRCAD Team An interview with Nicole Green, BSP, RPh, ACPR, DPLA, Director of the Ambulatory Pharmacy Services Program at ThedaCare, a healthcare organization based in northeastern and central Wisconsin serving both rural and urban areas. By: Aanchal Gupta, Program Coordinator, NaRCAD Tags: Program Management, Detailing Visits, Opioid Safety  Aanchal: Hi Nicole, thank you so much for talking about your program with us today! You’re a pharmacy director at ThedaCare—tell us more about the academic detailing component of your programming. Nicole: During the past four years working at ThedaCare, I’ve been studying ways in which pharmacists could serve as academic detailers to support opioid stewardship initiatives in order to positively influence prescribing. I was able to collaborate with other physician leaders as well as executive leadership who supported the program, gather data on opioid prescribing, and work on a proposal for academic detailing. We created our first formalized detailing project, called the Ambulatory Pharmacy Services Program, in January 2021. We had four detailers kick off our program and we’ve now doubled our team with a total of eight detailers that have all been trained by NaRCAD. Our detailers are ambulatory pharmacists who are embedded in ThedaCare’s family medicine and internal medicine clinics, serving as both medication experts and pharmacy consultants for patients and providers.  Aanchal: It’s incredible how quickly your program grew! Can you tell us more about the areas you’ve been focusing on for academic detailing? Nicole: Opioid stewardship is our main focus area for our detailing initiative. Our detailers identify patients who are candidates for Naloxone and work with clinicians to provide education to patients and their family members. The detailers also assess patients who have been on opioids for a long time and determine if they still need to be on them or if tapering should be considered. The second focus area is comprehensive medication management services for our self-insured population. This includes having our detailers identify chronic disease management gaps and partner with our state employees to optimize care for patients to reduce cost and readmissions. Our last focus area is to support our new heart failure clinic. Patients are referred to this clinic if they’ve been discharged from the hospital with heart failure or if they’ve been referred by a cardiologist. On initial visits, patients see a cardiology provider followed by an ambulatory pharmacist. Our role is to review the patient’s chart and provide recommendations to the team, as well as education to the patients. Our goals are to decrease readmissions and improve guideline-directed medical therapy.  Aanchal: Wow - your team’s impact is tremendous. You previously mentioned that you were able to double your detailing team in less than a year. What characteristics do you believe are needed to have a strong detailing team? Nicole: Having in-depth knowledge about the clinical topic is extremely important. Detailing is also about building trust and strengthening the relationship with confidence. Detailers need to be confident, especially when they’re first starting out and are meeting with providers that they have yet to build a relationship with. Detailers also need to be prepared to respond confidently and in a way that will still engage the providers in an open conversation. Providers typically don't understand that ambulatory pharmacists’ jobs are to assist patients to meet medication-related goals. There have been assumptions about why we’re delivering this service or why we’re meeting with clinicians. Clinicians ask questions such as, “Is it because I’m being targeted?” or “Is it because of my prescribing practices?”  Aanchal: Agreed; at NaRCAD, we know that having both clinical expertise and confidence communicating is essential to detail successfully. We know what makes a successful detailer – now let’s talk about what qualities you believe make you successful as a leader. Nicole: The first quality that comes to mind is passion. I lead with energy and show my team how exciting this work can be. I think that's important because previously we didn’t have pharmacists embedded in primary care and patients didn’t have an option to book an appointment with a pharmacist for consultation. Our pharmacists are delivering a service that was not there before. They need to promote themselves and make others aware of how they can help. Also, I like to be a strong advocate for my team. I constantly raise my hand saying that we can help with different initiatives or that certain projects are right up our alley.
Finally, I encourage my team to be persistent. We can't take the first “no” from a clinician as rejection. It might mean, “not now,” “I don't understand,” or “I haven't been exposed to this.” It doesn’t mean that they never want to have a visit with an academic detailer or will never change their prescribing behavior. Aanchal: These are all core elements in building a strong team. Some situations can feel defeating and having a strong leader that has your back is so important. Lastly, what advice do you have for someone who is new to managing a team of detailers? Nicole: Prepare your detailers for the field with the most up-to-date clinical content so that they can interact with clinicians confidently. Also, provide your detailers with training opportunities and use resources like NaRCAD. If you have the capacity, take it one step further by adding practice role play sessions among peers and allow new detailers to observe other detailers in the field. When training, help the detailers step out of their comfort zone within a group of people that they know before they step out of their comfort zone with a stranger. Aanchal: Yes, having support and receiving feedback from peers is an important element of building a strong team. Thank you so much for sharing your perspectives with us, Nicole! We look forward to continuing to see your team grow and feature your work at our upcoming conference! Have thoughts on our DETAILS Blog posts? You can head on over to our Discussion Forum to continue the conversation!  BIOGRAPHY: Nicole Green completed her pharmacy education at the University of Saskatchewan, Canada followed by a hospital residency. She practiced for over a decade as a Clinical Coordinator primarily in the area of cardiology. She has completed year-long learnings through the AIMM (Alliance for Integrate Medication Management) collaborative as well as the ASHP PLA (Pharmacy Leadership Academy). She is the Director of Ambulatory Pharmacy with ThedaCare. She leads the comprehensive strategic plan to embed pharmacists within family and internal medicine clinics as providers and vital members of the primary care clinical team. She has served as an Executive panelist with GTMRx (Get the Medications Right) and the Institute for Advancing Health Value.
Her program utilizes Academic Detailing as a means of building professional relationships, establishing credibility and influencing prescribing improvements. Much of her team’s work is related to Quality improvement initiatives in medication stewardship and safety as well as maximal performance in Pharmacy related ACO measures. Nicole has worked with the ThedaCare cardiology team to build a collaborative Heart Failure Clinic where patients see both a cardiology provider and am ambulatory pharmacist.  This series features tried-and-true practices from our AD experts. This week’s guest blogger is Zack Dumont, BSP, ACPR, MSPharm a NaRCAD Facilitator and Academic Detailer at RxFiles Academic Detailing Service. Curated by Anna Morgan-Barsamian, MPH, RN, PMP, Senior Manager, Training & Education, NaRCAD Tags: Detailing Visits, Stigma, Training  Model the compassion you expect from others. In recent years, the academic detailing community has been trying to recognize the harmful role of stigma in many clinical settings and to include stigma reduction in our detailing messages. In applying this framework, we encourage an empathetic view of people who experience stigma. They don’t choose to have addictions, exhibit certain behaviors, or to be ‘villainous’. We can all agree they don’t deserve harsh judgment and criticism. I invite you to bring forth your most charitable mindset for a moment and apply that same framework when you encounter stigma during a detailing visit. Imagine that the clinicians or people you detail hold stigma not because they want to stigmatize others, but for some more relatable reasons: they’re impressionable, they’re naïve, they’re vulnerable. In the same way that a clinician wouldn’t expect someone with a substance use disorder to suddenly recover if harshly confronted, we can’t expect the person who stigmatizes to respond to similar tactics. Be patient, be persistent (after all, you care and want them to be their best selves), and be persuasive with those that you’re detailing. You have a lot of natural talent, training, and experience to efficiently help people make informed decisions through detailing visits. Don’t limit it to therapeutic decision-making; extend it to the mental and emotional aspects of care, as well.  Balance and refine your self-reflections. Alone or with a colleague, find a quick and easy way to debrief after each visit – save the more intense feedback for quarterly or annual reviews. Maybe it’s asking two simple questions like, “What went well?” and “What could have gone better?” and taking a moment to reflect on each. And, just like AD visits which are 90% prep and 10% execution, the more the better when it comes to ‘prepping’ your self-reflection questions. So, “What went well?” could be more specific to one of your strengths:
Your “What could have gone better?” question could focus on an area of improvement unique to you:
This isn’t easy, but it’s low risk with the potential for big reward… so I encourage you to jump in! Want more tips? Stay tuned for the next installment in our Words of AD Wisdom series, and reach out to the NaRCAD team, subscribe to our network, or check out our discussion forum to hear more tips and ways to train your brain!  Biography. Zack is a clinical pharmacist with the RxFiles Academic Detailing Service in Regina, Saskatchewan, Canada and an expert facilitator for NaRCAD's training courses. He has been involved with the RxFiles since 2008, with experience in both academic detailing and content development of RxFiles’ evidence-based drug therapy comparison tools. Zack also serves as the Clinical Manager for the Saskatchewan Health Authority Pharmacy Department. His practice has largely been hospital-based, with more specialized experience in anticoagulation and heart failure. His professional interests include evidence-based medicine, information technology, and leadership.
Zack graduated as a Pharmacist from the University of Saskatchewan in 2008. Following graduation, he completed a hospital pharmacy residency with the Regina Qu’Appelle Health Region. He also completed a Master’s degree in Pharmacy, with a focus on leadership, from the University of Cincinnati. By Anna Morgan-Barsamian, MPH, RN, PMP, Senior Manager, Training & Education, NaRCAD An interview with Lexie Hach, Regional Health Specialist, Bureau of HIV, STD, and Hepatitis, Capacity Extension Program, Iowa Department of Public Health. Tags: Detailing Visits, Evidence-Based Medicine, Stigma, Rural AD Program  Anna: Hi, Lexie! We’re excited to chat with you today about your detailing work in rural Iowa. Your program started about 5 years ago and was born out of the HIV and Hepatitis Community Planning Group (CPG). Can you share more about the CPG and how the detailing program was created? Lexie: The CPG is made up of healthcare providers, people with lived experience, case managers, educators, and other stakeholders. The group serves in an advisory capacity to the Bureau of HIV, STD, and Hepatitis at the Iowa Department of Public Health (IDPH) and their main task is to ensure that the state has an inclusive participatory planning and evaluation process for the delivery of prevention and care services. About 5 years ago, the CPG recognized a need for more education in the rural parts of Iowa related to best practices in HIV, sexually transmitted infections (STIs), and Hepatitis. That’s when we learned about AD. We started building our detailing program based on a lot of the work that New York City’s program was doing. We now have 5 detailers, who we call Regional Health Specialists (RHS).  Anna: What an interesting start to your program! You’re currently assigned to detail in 15 counties in central Iowa covering over 20 sexual health topics, from stigma to your statewide condom program to new screening recommendations. Do you detail on these topics beyond the primary care setting? Lexie: Yes! Our goal as detailers is to provide the best health outcomes for people living with HIV and those living with, or at risk for, STIs and Hepatitis C. We meet with the medical community including, local health departments, community-based corrections, substance use specialties, mental health, and many community based organizations. We also attend a variety of community meetings. We know that many people living with HIV pass through community-based organizations. We want to make sure that those organizations are equipped with the correct information to get people the care they need through resources or referrals. Our team has created detailing materials for both medical professionals and community-based organizations to maximize our impact. Anna: Working with community-based organizations is a great way to make sure people have access to the best possible prevention and care, especially in a rural state like Iowa. How does Iowa’s geography impact your detailing work?  Lexie: Iowa has 3.1 million people with about 54 people per square mile. Our state is 85% farmland with country roads, winter weather, and a lot of construction. It is not uncommon to lose cell service or your GPS signal while driving in the very rural parts of Iowa. We’ve adapted our detailing approach because of this and have found that group sessions work best for us. We identify champions in the clinics and are then able to set up 1:1 visits with clinicians as needed. Anna: We often hear from programs that group detailing is a great way to get your foot in the door and spread the word about AD. It’s nice to know that it’s working so well for your program too! I imagine Iowa’s geography also impacts patient care. Lexie: Yes, it does. There can be stigma around seeking sexual health care in rural parts of Iowa. Many times, patients know someone working at the clinic in their town. It’s common for patients to travel long distances to get to a clinic where they don’t know anyone. It’s also common for patients to have to travel over 2 hours to access HIV care at a specialty clinic. Anna: And that’s 2 hours one way! Has your program been able help with increasing access to care? Lexie: Yes, I can share one story that stands out the most to me. A couple of years ago, I was presenting at a community meeting with 15 or so people in attendance. The CEO of a federally qualified health center (FQHC) in Southern Iowa was also present and we were able to connect and network afterwards. We talked about how far patients must travel for Ryan White HIV care and he saw a need that the community health center could fill. We connected with senior leadership, there were additional meetings, and together we were able to bring Ryan White HIV care services to the health center. Those services are still there today and now people living with HIV in Southern Iowa can access Ryan White services closer to home. Anna: There is so much to be said about the power of AD, networking, and champions! Let’s wrap up with hearing about some of your program’s successes from this past year. Lexie: We’re so proud of all that we’ve accomplished this year! Here are some highlights:  Anna: Those are some impressive numbers across both the clinical and community settings. Thank you for letting us feature your detailing work and learn more about the impact your team is making in your state! Have thoughts on our DETAILS Blog posts? You can head on over to our Discussion Forum to continue the conversation!  Biography. Lexie Hach holds an Associate Degree in Nursing, Bachelor of Arts degree in Health Promotion and Women’s Health, and a Master of Arts degree in Community Health Education. Lexie is currently a Doctoral student in Public Health (DrPH) with an Epidemiology concentration at the University of Nebraska Medical Center (UNMC).
Lexie has held positions in nursing, health education, public health, and healthcare marketing. Lexie has been with the Bureau of HIV, STD, and Hepatitis Capacity Extension Program at the Iowa Department of Public Health for over five years as a Regional Health Specialist (RHS). Lexie was previously with the bureau as a Disease Intervention Specialist (DIS). Lexie was instrumental in developing and implementing the RHS program in Iowa’s rural communities. In her RHS (academic detailing) role, Lexie educated a variety of different stakeholders on best practices related to HIV, STIs, and Hepatitis in central Iowa. Lexie has helped support the Sexually Transmitted Disease (STD) Program as a DIS due to COVID-19 and also helped as a COVID-19 contact tracer. Lexie was the previous workforce health department co-chair for Iowa’s statewide strategic plan to stop HIV in Iowa (Stop HIV Iowa). Lexie recently returned to her roots in the STD program and now serves as an Integrated DIS and Special Projects Coordinator, but continues to work alongside her fellow RHS colleagues. By Anna Morgan-Barsamian, MPH, RN, PMP, Senior Manager, Training & Education, NaRCAD An interview with Sandeep (Sonny) Singh Bains, PharmD, BCPS, Clinical Educator, Alosa Health. Alosa Health is a national leader in developing and implementing academic detailing programs to improve prescribing. Tags: Detailing Visits, Evidence-Based Medicine, Primary Care, Training  Anna: Hi, Sonny! It’s wonderful to connect with you today and hear about your work as a clinical educator at Alosa Health. What has your clinical pharmacist journey looked like to date? Sonny: I’ve been working for over a decade in hospitals and primary care. I completed my residency in hospital pharmacy, and as I continued to do administrative and clinical work in hospitals, my interests shifted more towards primary care and population health. I’m originally from California where it’s common to have pharmacy involved in primary care. When I moved to Pennsylvania, a lot of clinicians didn’t understand why a pharmacist would be in a primary care setting and were skeptical of me and my role within the clinic. Fast-forward 10 years, and almost every health system in Philadelphia has a pharmacist on their team within their primary care network. I’d like to think that I can take a little bit of credit for paving the way for pharmacists on primary care teams throughout our state! Anna: That’s definitely something to be proud of. How did you end up being a detailer?  Sonny: I’d been noticing a lot of overlap in the work being done in our primary care clinics by different members of the team. I ended up creating protocols to automate certain things for different chronic conditions and people would say, “Wow, this is brilliant.” It really wasn’t brilliant; I was using the same set of guidelines in the literature I was reading and was communicating that to clinicians to make workflows easier. I didn’t know about the strategy of academic detailing at the time, but I knew I needed to educate clinicians. I was fortunate enough to be connected with Alosa Health and I now work for them as a full-time consultant. I work as a detailer and also help hire, interview, train, coach, and mentor new detailers on the team. Anna: You were meant to be a detailer before you even knew what it was! Alosa has been working on diverse clinical topics over the years including, antiplatelets, atrial fibrillation, immunizations for elderly, serious illness conversations, chronic obstructive pulmonary disease (COPD), heart failure, dementia, atherosclerotic cardiovascular disease (ASCVD) prevention, diabetes, acute pain, chronic pain, and opioid use disorder. What have been some of the campaigns where you’ve felt you’ve made an impact? Sonny: It’s a lot of fun to be working on so many different campaigns. Many of the topics fit right into my wheelhouse with my hospital and primary care background. Diabetes has been my favorite topic. I’ve been able to make a large impact for patients and care providers. We’re able to improve lives of patients (prevention of stroke/heart attacks) and improve outcomes for providers and health systems (financial incentives, quality ratings, etc.). I’m also proud to be part of the pain modules. The opioid epidemic has impacted all of us in America and I’m glad to be able to do my part in helping to bring resources and evidence-based treatment to local providers in our community.  Anna: It sure sounds like you’ve been able to make an impact! How has your work with Alosa evolved over the years? Sonny: Alosa Health has been expanding and we have several new partnerships and collaborations throughout the United States. We started detailing only in the state of Pennsylvania and we’ve now expanded to numerous states. It’s been exciting to be part of the leadership team to help coach detailers, as well as create creative partnerships with local health systems to improve outcomes for patients. Anna: What challenges have come up as your program has continued to expand? Sonny: The biggest barrier we’ve experienced, like many detailing programs, has been access to clinicians and the ability to set up visits. I’ve had relationships with clinicians and clinic staff in the past where I could have walked into any office at any given time, but I’ve lost a lot of those relationships with COVID and staff turnover. I’ve been working hard to reestablish relationships in the field and teach new detailers how important strong relationships are to our work as detailers.  Anna: What approaches have you taken to reestablish relationships, as well as to gain access to new clinics? Sonny: I like to partner with colleagues that I’ve worked with previously. I recently connected with a former colleague who’s a VP at a large healthcare organization and we quickly realized we could help each other improve patient outcomes and reduce cost. From this connection, I was able to get buy-in at the administrative level and accessed hundreds of prescribers. They even gave their clinicians a monetary incentive to meet with our detailers. We’ve also benefited from connecting with administrators of health systems. We approach them like business partners; it takes a special skill to communicate and work with an administrator. It’s important to have team members who understand how to communicate with leadership effectively to get that buy-in. Anna: It might take more time to get buy-in from administrators, but it opens so many doors once it’s done successfully. As we wrap up, can you tell us some tips to help our readers be effective detailers and communicators? Sonny:
Anna: It’s so important to put the work in to build solid relationships with clinicians in order to be an effective detailer. Thanks for joining us on the DETAILS blog, Sonny - our AD community will gain a lot from the insights you’ve shared today! Learn more about Alosa’s work: alosahealth.org/clinical-modules Have thoughts on our DETAILS Blog posts? You can head on over to our Discussion Forum to continue the conversation!  Biography. Sandeep is a clinical pharmacist with extensive clinical leadership experience in both acute care and ambulatory healthcare settings. He completed post-graduate training at Einstein Medical Center in Philadelphia and has since worked in clinical pharmacy leadership with large healthcare systems in the greater Philadelphia area. He is also the principal consultant at Bains Rx, LLC, a healthcare consulting firm dedicated to improving outcomes while reducing costs.
An interview with Rachelle Woods, MSN, RN, Nurse Consultant at the Colorado Department of Public Health and Environment (CDPHE). By: Aanchal Gupta, Program Coordinator, NaRCAD Tags: HIV/AIDS, PrEP, Detailing Visit  Aanchal: Hi Rachelle! We’re so excited to learn more about the work you’re doing. To start, can you tell us about your background and your current role? Rachelle: I’ve been a registered nurse in the state of Colorado for 26 years. My clinical background is obstetrics and gynecology (OBGYN), which includes family planning, HIV/STI education, and direct patient care. I've also taught OBGYN and other health courses at a few nursing schools and universities as well as in the community. I've been at CDPHE for a little over three months and will be functioning as a nurse consultant and public health detailer. I'm currently working to harness a deeper understanding of the needs of each of the communities that I'll be serving within our state. In order to do that, I’ll be conducting a statewide community needs assessment. I plan to tailor the needs of each geographic area when detailing to identify areas of urgent need and take into consideration epidemiological concerns among special populations. CDPHE is implementing a public health detailing approach to control STI and HIV infections which are increasing in Colorado and across the nation. My role is to serve as both a recruiter and consultant to optimize healthcare integration of public health prevention practices regarding STIs, HIV, and viral hepatitis within our state.  Aanchal: It’s exciting to hear how your background intersects with your current role at CDPHE. I’m curious about the community aspect that you spoke about. What services and supports already exist in your community for the patient populations you’re working with? Rachelle: CDPHE has 80 contracts with several community-based organizations and local public health agencies throughout the state. Our goal is to collaborate across sectors and provide services within several of our communities. Our partners include pharmacies, pharmacists, clinical providers, non-clinical persons, public health agencies, publicly funded healthcare centers, and other community-based organizations.  A graph from CDPHE showing the number of clients who received a PrEP prescription from 2015-2018. A graph from CDPHE showing the number of clients who received a PrEP prescription from 2015-2018. Aanchal: It's important to leverage others in the community to provide the best care and support to patients. Tell us about CDPHE’s prior successes with HIV PrEP detailing. Rachelle: We had a public health detailer a few years back that focused on PrEP rollout. Between 2014 to 2019, PrEP use increased from 383 to 3,659 among Coloradoans. We’re now working on expanding our public health detailing program and have been focused on partnering with other local agencies to bring the best evidence to clinicians. The Denver Health and Hospital Authority has helped us disseminate relevant updates to providers so that we can better meet the needs of Colorado’s most vulnerable populations.  Aanchal: It’s impressive that your program had success with your first detailing intervention and that you’re continuing the momentum with a community-based approach to detailing. Since you began the role a few months ago, what resources helped you to learn more about academic detailing? Rachelle: I spent a great deal of time on the NaRCAD website and reviewing our internal resources. I was introduced to NaRCAD by my director, Rosemarie. She said, “I know that you have experience with educating clinicians, but I want you to take a look at this organization and see if perhaps there could be anything of benefit for you.” I spent a whole week absorbing the materials on the NaRCAD website. Being able to access the webinars and videos on demand was especially helpful. I'm somebody who likes to keep my finger on the stop button when watching a video so I can replay and relisten. I loved the fact that I could get a firm grasp of the concepts of AD at my own pace.  Aanchal: I’m glad you found the NaRCAD website to be useful as a new detailer. Based on that, if someone were in your shoes and was just starting out as a detailer, what advice would you give them? Rachelle: When you initially step into something new, you're outside of your comfort zone. Do you harness the fear and turn it into excitement for learning or do you shy away from it? It's important to step into it and remember that the goal is to better the communities that we live in. Take that excitement and run with it. Don't be afraid – as long as your intentions are in the right place, everything's going to work out. Aanchal: Definitely! I’m sure that’s a reminder many of us need to hear. Thank you so much for speaking with us, Rachelle! We look forward to hearing more about your findings from the community needs assessment and your exciting detailing project. Have thoughts on our DETAILS Blog posts? You can head on over to our Discussion Forum to continue the conversation!  Biography:
Rachelle Woods, MSN, RN brings an expansive clinical, leadership, and professional development background deeply rooted in OBGYN, STI/HIV, Family Planning, Transgender Health, and Infection Control to the Public Health Detailer role at CDPHE. Rachelle’s passion for all things infectious has afforded her a career rich in opportunity to meet people where they are and engage in robust discussion surrounding STI/HIV transmission, prevention, biomedical interventions and resources, and personal wellbeing. Her audiences have spanned multiple platforms and have included clinical and non-clinical staff, patients/families, teens, and students. Rachelle is looking forward to applying her skills and experience in support and growth of the Public Health Detailer role at CDPHE. By Anna Morgan-Barsamian, MPH, RN, PMP, Senior Manager, Training & Education, NaRCAD An interview with Trish Rawn, BScPhm, PharmD, Clinical Service Director and Academic Detailer, Centre for Effective Practice (CEP). CEP is a not-for-profit in Canada that aims to close the gap between evidence and practice for healthcare providers. Tags: Stigma, Detailing Visits, Substance Use  CEP's COVID-19 Resource Centre CEP's COVID-19 Resource Centre Anna: Hi Trish! Thanks for joining us today. Your team has been working on a number of AD campaigns including, falls prevention, type 2 diabetes, benzodiazepine use in older adults, chronic non-cancer pain (CNCP), and opioid use disorder (OUD). Can you tell us about some of the other recent work you’ve been doing at CEP? Trish: Our team’s academic detailing work is a big part of what we do, but CEP has other supports as well. We create clinical tools and resources on myriad clinical topics where practice gaps have been identified. Our most popular resource has been our COVID-19 Resource Centre to support primary care clinicians in adapting their practice during the pandemic. It’s become a massive resource that has had over 140,000 downloads. Anna: Wow! That’s an impressive amount of downloads. One of the other priority areas where your team has identified practice gaps is OUD. This topic often has a lot of stigma associated with it. Is this something you’ve experienced with the opioid detailing campaigns?  Trish: When we first started detailing on CNCP, opioid tapering, and OUD, there was a lot of fear and stigma among clinicians. They didn’t want to be known as the doctor “prescribing all the opioids.” Some clinicians were concerned that they might get in trouble, and they’d say things like, “I don’t have any of those patients” or “They’re all inherited patients.” Clinicians also sometimes felt like they didn’t want to say the wrong thing to patients, so they wouldn’t say anything at all. We’re all guilty of this and we’ve tried to encourage language like, “Hey, I might be saying the wrong thing here, but let's just start the conversation.” Anna: Just starting the conversation with the right intentions is helpful, even if you don’t get the language completely correct. Have you seen any stigma at the patient level? Trish: We found that patients themselves were experiencing stigma when seeking help and when trying to talk openly about opioids with their clinicians. Family doctors are in a vital position to help patients because they tend to have long-term, trusting relationships with them; they have sometimes taken care of them since they were children. Studies show that when opioid replacement therapy is prescribed by family doctors, there are improvements in patient uptake, patient satisfaction, and treatment success. We wanted to get the clinicians to a place where they felt confident talking with patients about opioids and where their patients felt comfortable sharing their experiences. It may feel like a jump for a clinician to go from, “I'm here to measure your blood pressure and adjust your medications” to “Let's talk about opioid addiction and set goals around tapering.”  CEP's Opioid Use Disorder Tool CEP's Opioid Use Disorder Tool Anna: I can see how talking about OUD might make some clinicians feel uncomfortable. What types of resources has your team developed to support both clinicians and their patients to feel more comfortable having these conversations? Trish: For our academic detailing visits on opioids and CNCP we developed a resource called Talking Points with Patients, which includes scripts for clinicians to handle different scenarios. For example, one of the scenarios is about a patient asking for a dose increase for an opioid, but the clinician not agreeing that a dose increase will help manage their pain. We also have a Specific, Measurable, Achievable, Relevant, and Time-Bound (SMART) Goals resource to help clinicians set goals with their patients by taking the focus off the pain number scale and focusing on actions like, “What activities would you like to do if you had less pain?” Anna: It’s clear that your team works hard to develop and tailor resources to support clinicians and patients. What kinds of local resources from your community are available for detailers to share with clinicians? Trish: We often help clinicians find local resources through a program called The Healthline, which is a website that connects patients with social supports, like counseling, food, and safety. We’re also lucky to have Rapid Access Addiction Medicine (RAAM) clinics in our community that are a one-stop shop for patients with OUD where they’re assessed, given support and a plan for tapering, and referred to other community services. Anna: It’s so important for clinicians and patients to be linked to local resources and know that they have a community supporting them. Can you share some data about how clinicians reacted to the opioid-specific campaigns overall?  Trish: Absolutely! I can share some key findings from our opioid campaigns. Opioid therapy for CNCP AD campaign (n=475): After the detailing sessions, clinicians indicated they were confident in their ability to have a conversation about tapering when appropriate, even when the discussion was challenging (93.5%). Non-pharmacological and non-opioid alternatives for CNCP AD campaign (n=323): Clinicians indicated that after the detailing sessions they were confident in their ability to help patients:
OUD AD campaign (n=250): Clinicians indicated that the detailing sessions enabled them to support patients with OUD by:
Anna: That’s incredible. It’s obvious that your campaigns have made a huge impact on clinicians. What advice would you give to other AD programs who are supporting clinicians in reducing stigma, especially as it relates to opioids? Trish: I would recommend remembering three key points: Examine your own biases: When developing detailing tools, you need to make sure that you’re aware of your own biases and that your tools include the lens of equity, diversity, and inclusion. This is something we are actively working on incorporating in all our work at CEP. Make space for clinician experiences: It’s important to remember to be sensitive to the clinician perspective. There have been times, especially with opioids, where clinicians have had painful experiences with patients overdosing. Be aware of their perceptions and respectful of the trauma they may have experienced. Know your patient population: Understand who the patients are, the trauma they’ve faced, and the stigma they may endure. Look at the experiences of your team, the clinicians, and the patients you’re working with and try to understand how these different perspectives all influence one another as you develop your resources. Anna: That’s beautifully said, Trish. Thank you so much for sharing about your important work in reducing stigma around OUD. Have thoughts on our DETAILS Blog posts? You can head on over to our Discussion Forum to continue the conversation!  Biography. Trish Rawn is the Clinical Service Director for the Centre for Effective Practice Academic Detailing Service. She is a hospital pharmacist who has been detailing for 6 years on topics such as antipsychotics in the elderly, opioid tapering, chronic pain, diabetes, falls prevention, and benzodiazepine deprescribing.
By Anna Morgan-Barsamian, MPH, RN, PMP, Senior Manager, Training & Education, NaRCAD An interview with Adrienne Butterwick, MPH, CHES, Senior Improvement Advisor and Academic Detailing Project Manager, Comagine Health. Comagine Health is a national, nonprofit, health care consulting firm that works collaboratively with patients, providers, payers and other stakeholders to reimagine, redesign and implement sustainable improvements in the health care system. Tags: Detailing Visits, Evidence Based, Substance Use, Opioid Safety  Anna: Hi Adrienne! We recently saw you present on a panel where you spoke about your academic detailing project with dentists on opioid safety. Can you tell us a little more about how your team got started with this work? Adrienne: In 2018, the CDC released funds to states through the Overdose Data to Action (OD2A) grant and the state of Utah selected academic detailing as one of the interventions they wanted to use. AD is one of the many different modalities that we use within my organization to reach clinicians to educate them and have an impact on the kind of care they provide. The state began looking at specific regions and populations to target after we received the funding. Utah is unique in that it has a high number of adolescents undergoing surgery for wisdom teeth removal, which is one of the most common instances where controlled substances are prescribed. A first prescription can be a huge turning point to potentially becoming addicted to a substance, especially at a young age. That’s when we decided to put together a team of two detailers to detail dentists. I was lucky enough to attend each detailing visit and collect data through pre- and post-surveys and answer any administrative questions that came up.  Anna: It’s impressive that your organization was able to look at the data in your state and build a program to fill a specific care need. What makes dentists and their environments unique when it comes to detailing? Adrienne: There’s a theory that providers who are prescribing controlled substances are working within systems and teams that are well-poised to understand the challenges of opioid prescribing. Dentists fall into a different healthcare model that’s often siloed; they aren’t usually affiliated with an overarching health system or university like many primary care providers are. This results in isolation, making the interactive, 1:1 outreach model of detailing even more important – we knew we needed to bring the information and support directly to them in their dental offices. Anna: Detailing seems like a critical need for isolated dentists, both in providing them with customized education, but also in building connections. Were there any special considerations that your team took into account as you worked with the dentists? Adrienne: The language that’s used in the dental world is very different than language that’s used in primary care. We were fortunate enough to have a dental provider, who’s a champion of AD, work with us as a detailer on our project. He knew the language, understood the workflow, and could speak to the need for safe opioid prescribing. He always started his detailing sessions with a personal story like, “When I took wisdom teeth out, I would always prescribe 40 Percocet pills. All I can think of today is, ‘what have I done?’” You could see the mood shift the moment he started talking about his personal experiences, allowing for a connection between himself and the dentists he met. The success of this program wouldn’t have gone even half as far without his support.  Anna: A detailer who can build empathy with clinicians and who has personal experience with a challenging topic is an important asset to have in a detailing program. What obstacles did you face as your team implemented this project? Adrienne: Connecting with dental offices, in general, was tough. We first started by working with dental associations to get relationships in place. We submitted newsletter articles, attended meetings, presented at the regional conference, and sent our program’s information via their listservs. We also Googled practices and found ones that had more than one dentist working in the office at a time. We’d cold call those offices and say, “It looks like you have a big operation – is there a way we could bring training in for your team for continuing education credits?” Before leaving the visits, we’d ask the dentists for referrals to other clinicians and leave flyers behind. Relationships grew organically over time. Anna: It sounds like the project began to build on itself fairly quickly. Did your team experience any barriers from the dentists during the detailing visits? Adrienne: We had a lot of dentists who thought the opioid crisis wasn’t relevant to their practice and we knew that we had to find ways to tie it into their profession. Fortunately, dentists have historically been involved in public health movements because they hold a different type of relationship with patients that is closer than a typical relationship with a primary care provider. They see patients more frequently and can detect small changes in health quickly. The dental profession was incredibly important in the tobacco cessation movement in the 1990s. They were instrumental in getting individuals to reduce or completely stop using tobacco. Dentists are also starting to be trained in domestic violence and human trafficking. For the dentists who were hesitant about the relevance of our detailing visits, we would say, “You have this amazing relationship with patients that we don’t see in other parts of healthcare—here’s how you can make a huge difference!” or “I can understand how there would be a lot of fear to step out of your comfort zone; we have a lot of resources and materials to support you.”  Anna: Dentists truly have a unique relationship with patients that can be used to promote countless public health initiatives. Can you think of a time your team was able to empower a dentist to change behavior and encourage them to see their relevance in combatting the opioid crisis? Adrienne: There was a dental group in a rural part of the state that had one dentist and a big support staff. We came in for a detailing visit and had a conversation with the entire office. After the meeting, one of the dental assistants pulled me aside and told me that a patient who had recently completed substance use rehab had visited the office in need of a procedure that would warrant prescribing an opioid. No one in the office knew what to do for pain control and they were all unsure how to approach the patient given his history. She said that because we came, she felt like she now knew how to have a conversation with him about the procedure and his safer, alternative options for pain management. The dentist also shared that prior to our visit, he often didn’t know how to handle conversations about pain management and opioids and wasn’t sure if it was his job to do so. After our visit, he said he felt comfortable and confident doing this, and shared an anecdote of being able to create a safe space for an ongoing conversation with a recent patient. Anna: It seems like your team has had such an impact by using one of the core elements of detailing – building relationships through empathy, validation, and support. Can you share some encouragement for readers who are considering having these conversations with dentists? Adrienne: Be flexible and don’t come in with your own agenda – be sure to let the dentists drive the conversation and let them teach you along the way. It can be a rewarding yet challenging experience – don’t forget to celebrate the small wins on your journey! Anna: Thanks for sharing this innovative approach to detailing, Adrienne! We’re looking forward to hearing about your continued impact with the dental community and beyond. Have thoughts on our DETAILS Blog posts? You can head on over to our Discussion Forum to continue the conversation!  Biography. Ms. Butterwick is a Senior Improvement Advisor at Comagine Health. She is currently working on quality improvement efforts directed by the Centers for Medicare & Medicaid Services (CMS) to improve quality of care for residents living in post-acute and long term care as well as assisted living and home health. She's also working on an initiative to increase advance care practices in those settings.
In addition, through a subcontract with the Utah Department of Health, Ms. Butterwick currently provides educational support for opioid prescribing to family medicine and dental providers. Her work with this contract has earned national recognition and has been presented at the RX Drug and Heroin Abuse Summit in April 2020 and the American Public Health Association’s annual conference in October 2020. She is currently also collaborating with faculty from the University of Utah regarding telehealth and advance care planning initiatives through the Utah Geriatric Education Consortium and Geriatric Workforce Enhancement Programs. She completed her Bachelors of Science degree in Behavioral Science and Health at the University of Utah in 2007 and her Master's in Public Health at Westminster College in 2014. She has also earned recognition as a Certified Healthcare Education Specialist (CHES). In her 15 years of public health project management she has also worked in rural health research, provider education programs and care management. She has a strong passion for quality improvement and public health.  Words of AD Wisdom is a series that features tried-and-true practices from AD experts. Our guest blogger this week is Chirag Rathod, PharmD, a NaRCAD Facilitator and Academic Detailer at Illinois ADVANCE. Tags: Detailing Visits, Evidence Based Medicine, Materials  Simplify your messaging! Prior to your detailing visit, think about ways to slow down and limit the amount of information you share with the clinician so that the visit is of most value to them. You can do this by asking focused needs assessment questions and providing the clinician ample opportunities to speak and engage in the conversation.  Focus. Focus. Focus. Resist the urge to cover too much content in your detailing aid during an AD visit. A more focused discussion on one section of your brochure can be more fruitful than trying to cover every key message during a single visit.  Open-ended questions will set you free! There is limited usefulness in asking closed-ended questions (e.g., confirming something about the clinician’s practice). The use of open-ended questions can help you gain layered insight into the clinician’s practice and tailor the visit to them. Asking open-ended questions allows opportunities for the clinician to speak about their experiences in detail and for you to listen and deliver supportive, relevant key messages.  Prime your “AD Kitchen.” In cooking shows, hosts show you how to prep a meal, pulling out the final, cooked meal from the oven in the following scene. For an AD visit, you should think about how you can prep your ‘ingredients’ for clinicians by making sure you’re well-versed in your materials and are ready to teach your clinicians how to adopt something practical and usable into their practice. Have a tool to share? Test it in advance of your visit, so you can confidently demonstrate effective use of the tool, leaving more time to discuss applying the tool successfully in practice with patients. Want more tips? Stay tuned for the next installment in our Words of AD Wisdom series, and reach out to the NaRCAD team, subscribe to our network, or check out our discussion forum to hear more tips and ways to prime your AD kitchen for an efficient visit!  Biography. Chirag is a clinical pharmacist, academic detailer and instructor with Illinois ADVANCE at the University of Illinois-Chicago (UIC). He graduated with a Doctor of Pharmacy degree from Midwestern University in 2012 and has been working at UIC ever since. During his time at UIC, he has been involved in a number of collaborations with the College of Pharmacy, College of Dentistry, and College of Medicine in addition to teaching Medical Improv, which utilizes the techniques of improvisation to improve communication skills amongst current and future healthcare practitioners.
He has also been focused on academic detailing, including program planning, presentations to recruit organizations, creating educational material, training staff, facilitating role plays and providing individualized feedback, and detailing prescribers. He trained with NaRCAD in 2019 during their Spring Training Series to develop his skills as an academic detailer and has also presented at the NaRCAD annual conference. His interests include performing improv, podcasting, sports and hanging out with his sister’s dog. Fun fact: Chirag hiked Mount Kilimanjaro in February of 2022.  We’re featuring a snapshot from academic detailer, Carolyn Wilson, a Senior Health Program Coordinator at Ledge Light Health District. By Anna Morgan-Barsamian, MPH, RN, PMP, Senior Manager, Training & Education, NaRCAD Tags: Substance Use, Detailing Visit  Anna: Hi Carolyn! Can you walk us through how you gain access to clinicians? Carolyn: Absolutely! When it comes to finding clinicians and getting them interested in our program, it’s really all about word of mouth. The clinicians quickly learn that the information I share is valuable and that I’m respectful of their time. I say things at the end of our visit like, “if you really enjoyed this session, the best compliment that I can receive is a referral to somebody else.” A referral or warm handoff always seems to work for me when gaining access. I also do a little bit of cold calling on LinkedIn - I share information about our program and attach our flyer. I make sure to mention our continuing education credits, referral gift cards, and swag. Clinicians absolutely love our insulated travel mugs. We’re fortunate enough to have the funding to provide these incentives through our grant. Once I’m 1:1 with a clinician, I always try to set the stage during our first meeting, especially if I don’t have a relationship with them. I let them know that I’m a non-clinical health educator and that I have a background in public health. I like to say that I’m a health promoter, not a clinician. I tell the clinician I’m working with that they know how to do their job, but I’m there to support them. I always thank them for their interest and time, which helps to build that relationship and open the door for follow up visits. Bottom line - entice people and let them know your value! At the end of the day, you want clinicians to know that you’re there to help them and that they can access you whenever they need support. Have thoughts on our DETAILS Blog posts? You can head on over to our Discussion Forum to continue the conversation! Biography. Carolyn Wilson is a health educator and prevention specialist serving as a program coordinator at Ledge Light Health District in New London CT for 11 years. Carolyn studied public health and health education at New York Medical College. Keenly interested in health promotion and behavioral science, Carolyn enjoys bringing her passions and talents to both primary prevention and academic detailing work. Carolyn has been serving as an academic detailer for over 2 years and enjoys speaking with clinicians about strategies to prevent opioid related deaths. Carolyn also manages the Groton Alliance for Substance abuse Prevention @Groton_Prevents. In her spare time, Carolyn enjoys serving on the Board of Directors for the CT Association of Prevention Professionals and Fiddleheads Food Cooperative. To connect with Carolyn, find her on LinkedIn.
By: Aanchal Gupta, Program Coordinator, NaRCAD Tags: Detailing Visits, CME, E-Detailing You asked, we answered! Getting your foot-in-the-door to schedule a detailing visit is a challenge for many detailers. We’ve compiled some of our best tips about gaining access from our past interviewees on the DETAILS blog.  Relationship Building:
 Incentives:
Tools:
Our team at NaRCAD recognizes the difficulties detailers face in getting the 1:1 visit, and we’re here to support you! Check out the list below for more resources on gaining access. Additional Resources on Gaining Access:
Have any additional questions or thoughts on gaining access? Write to us in the comment section below! Peer-to-Peer Learning: Building Meaningful Relationships through NaRCAD’s Peer Connection Program2/7/2022
An interview with Cheryl Radeloff, Senior Health Educator at the Southern Nevada Health District in the Office of Disease Surveillance. By Aanchal Gupta, Program Coordinator, NaRCAD Tags: Detailing Visits, HIV/AIDS, PrEP Aanchal: Hi Cheryl, we’re looking forward to hearing more about your experience in the NaRCAD Peer Connection Program! How did you hear about the program and what encouraged you to sign up? Cheryl: I found out about the 2021 Peer Connection Program from a NaRCAD e-blast and was intrigued with the idea of joining a learning community. I instantly knew that I wanted to sign up since it would be a place where I could feel comfortable asking questions. I gravitated to the fact that I would be communicating with other peers in the field during cohort gatherings and learning about approaches that we could emulate in our program.  Aanchal: Yes, having that 1:1 time with your peer, as well as the cohort gatherings where other participants in the program come together, are added ways to network with the detailing community. Would you recommend this program to others that are interested in signing up? Cheryl: Absolutely! You should sign up even if you're a seasoned academic detailer or new to detailing. You're going to get tips, insights, and resources to get you started in a welcoming environment. This is a field where you never stop learning so it’s not only an opportunity to share lessons learned, but to learn from others as well. There are people from across the world who have different experiences and expertise that you can take back to your program.  Aanchal: One of the special aspects of the program is the sharing of resources and ideas. Are there any conversations that you had with your peer that made an impact on your detailing work or changed the way you thought about your program? Cheryl: The time spent with my peer was invaluable. During changing times with COVID-19, it can be daunting, and you tend to wonder if you’re doing things right or where you should even start. She was so generous in talking through challenges such as funding, recruiting providers, and more with me. She even shared a PowerPoint that they developed to educate pharmacy students about academic detailing. During the mid-point peer connection gathering, I was able to learn about a program in Chicago. They were very innovative; if they didn’t have an approach in place for their program, they designed it. Although my clinical topic may not be the same as others, there are still concepts and tools that I can model after these programs.  Aanchal: It’s great to hear about these fruitful conversations you had and how there’s always something to learn from others in the detailing community. How would you describe your experience overall with the peer connection program? Cheryl: Every time I attended a peer gathering, I always learned something and never had to question what I was gaining from these meetings. I think it’s essential to hear about what’s going on in the field. It’s difficult as we’re all busy people, yet it’s important not only for learning and development, but a necessary element to have peers to consult. I found the structure of this program to be helpful as we were given the reins to set up 1:1 meetings with our peer match over several months. In addition to that, there were gatherings where the entire cohort could come together and connect which I appreciated. 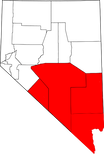 Aanchal: Those are some great takeaways, and we are glad to hear about the impact the program has had on your work! To wrap up, we’d love to learn more about what you’ve been up to at the Southern Nevada Health District. Cheryl: I’ve been with the Southern Nevada Health District for 13 years. Along with being a detailer, I’m also the public health co-chair for our HIV prevention planning group. We meet a few times a year to talk about HIV prevention initiatives, as required by the CDC. I also work with many of our community-based organizations to talk about the fundamentals of HIV. Academic detailing has been an important strategy for the work that we do. Our main AD initiatives we've been working on are uptake of PrEP and PEP. We have two PrEP navigators who've been educating the community about these initiatives. Lastly, congenital syphilis has been a big topic for us as we’re currently fourth in the country for the highest rates of syphilis. Aanchal: Thank you so much for sharing your experience, Cheryl. We’re so glad that the Peer Connection Program has had a positive impact on your detailing work and can’t wait to hear more about your program’s AD initiatives in the future. We look forward to continuing these connections with our 2022 cohort! Have thoughts on our DETAILS Blog posts? You can head on over to our Discussion Forum to continue the conversation!  Biography: Cheryl Radeloff is currently a Senior Health Educator with the Southern Nevada Health District Office of Epidemiology and Disease Surveillance. Formerly she was Disease Investigation and Intervention Specialist II. She is also an adjunct professor of Sociology at UNLV as well as Women’s Studies at the College of Southern Nevada. She received her Ph.D. in Sociology from the University of Nevada, Las Vegas in 2004. Her dissertation “Vectors, Polluters, and Murderers: HIV Testing Policies toward Prostitutes in Nevada” explored the development of mandatory testing laws for legal and non-legal sex workers in the state of Nevada. Her work duties include serving as the public health co-chair for the Southern Nevada HIV/AIDS Prevention Planning Group as well as training community providers on Rapid HIV Testing. She is the co-author of multiple editions of Transforming Scholarship: Why Women’s and Gender Studies Students are Changing Themselves and the World with Michele T. Berger for Routledge Press.
The Impact of Childhood Experiences on Patient Health: AD to Encourage Trauma-Informed Care1/31/2022
By Anna Morgan-Barsamian, MPH, RN, PMP, Senior Manager, Training & Education, NaRCAD  As we’ve jumped right into 2022 programming, our team at NaRCAD continues to support detailing efforts that improve outcomes for vulnerable populations, recognizing that patient needs are complex and often informed by social determinants of health. One critical topic for which we’ve developed resources focuses on detailing to improve patient health as informed by both adverse and positive childhood experiences. We’re seeing an increased need from our community members to support detailing efforts related to this critical topic. We partnered with the National Association of County and City Health Officials (NACCHO), Centers for Disease Control and Prevention (CDC), and consultants from Brigham and Women’s Hospital and Tufts Medical Center over the past two years to develop academic detailing materials for clinicians working with both adults and children. The CDC defines adverse childhood experiences (ACEs) as traumatic events that occur in childhood, including abuse, neglect, and family dysfunction. These events are linked to poor health outcomes in adulthood like chronic health problems, mental health conditions, and substance use. When considering the impact of environment on health, the CDC notes that children are likely to flourish when they have safe, nurturing relationships. These supportive settings create the opportunity for positive childhood experiences (PCEs). PCEs can mitigate the effects of ACEs and toxic stress, promote healing from traumatic events, and foster healthy development and learning in children.  Encouraging clinicians to consider both ACEs and PCEs is a natural fit for clinical outreach educators. There are many reasons that clinicians may not be prepared to have conversations with patients about childhood experiences. Perhaps the clinician doesn’t have a behavioral health provider to consult within their practice, so they don’t know who to turn to if a patient discloses a traumatic experience. A detailer can encourage a clinician to explore this concern, as well as provide a list of local behavioral health providers in the community. Another barrier may be that clinicians could feel hesitant to approach discussions related to trauma, or may not have the skills to do so with sensitivity. In this case, detailers can offer tools that illustrate supportive language that creates a safe environment for patients to share their experiences. Supporting clinicians in using evidence-based tools to build trust with their patients signals that it’s not only okay to talk to patients about this sensitive topic; it’s vital for clinicians to lead these conversations in order to ascertain their patients’ needs and promote patient-centered decision making. A detailer can encourage clinicians to adopt new behaviors through specific key messages, including asking clinicians to take the following steps to support adult patients:
 When clinicians are supporting pediatric patients, detailers can deliver this set of evidence-based key messages, encouraging clinicians to:
 With evidence-based tools, successful AD interventions related to ACEs can result in multi-faceted support for patients, such as stronger connections with community resources, mental health supports, and more trusting relationships between clinicians and their patients. We hope to continue to explore this important and complex topic together as a community. If your program is currently working on an ACEs or PCEs AD campaign, or is interested in starting one, please reach out to us so we can support the development of your programming. We always love collaborating and learning more about the important work that you’re doing, and we hope to continue to build our resources and create toolkits in support of complex topics such as these that intersect with other behavioral health and prevention-focused AD campaigns. Have thoughts on our DETAILS Blog posts?
You can head on over to our Discussion Forum to continue the conversation! |