The DETAILS BLOG
Capturing Stories from the Field: Reflections, Challenges, & Best Practices

 Tags: Autism, CME, Conference, Detailing Visits, Pediatrics, Practice Facilitation, Training NaRCAD: Hi, Meagan and Mindy—thanks for taking the time to talk with us about your clinical outreach education programming at Colorado ABCD. Can you give us an overview about ABCD and its mission to improve child development? Meagan Shallcross: Colorado Assuring Better Child Health & Development (ABCD) works with community partners, pediatric healthcare providers, early learning providers, and families across Colorado communities. The goal is to strengthen systems and identify children with developmental delays, connecting them with community services as early as possible.
 Meagan Shallcross, MPH Meagan Shallcross, MPH NaRCAD: Tell us a bit about your backgrounds. How did you each get into healthcare improvement? Meagan: My background in public health, along with experience working in clinical settings and behavioral science research, developed my interest in healthcare improvement that aims to bridge community work and clinical practice, standardize clinical workflows, and ultimately improve experiences and outcomes for patients and families  Mindy Craig, PA-C, M.S. Mindy Craig, PA-C, M.S. Mindy Craig: My path to healthcare improvement is a little different than what you might expect. I worked for Northwest Airlines as a flight attendant for several years straight out of college. At that time the airline industry was losing a large amount of money and needed to find a new way of operating. They decided to utilize a Total Quality Management approach and enlisted people from every department to undergo training in TQM and then facilitate small departmental groups in quality efforts. It was through this process that I began to understand the importance of doing business with a quality framework.  Learn more at coloradoabcd.org. Learn more at coloradoabcd.org. Eventually, I left Northwest and started working in a Neurology clinic while going back to school with the goal of becoming a PA. After completing my degree I worked in primary care settings for about 10 years. I participated in small clinic QI efforts over the years and continued to be interested in quality improvement. I was hired by ABCD 8 years ago to bring a clinical perspective to their physician outreach. It was a natural progression for me to start approaching our work at ABCD with a quality improvement framework. The power of engaging front line staff to implement changes that result in improvement remains as strong as it was when I worked in the airline industry. NaRCAD: Talk with us about your academic detailing programming at ABCD—you’ve been doing this for about 10 years, right? Mindy: We started our work encouraging the use of standardized developmental screening tools in the primary care settings. This was supported by the American Academy of Pediatrics policy statement in 2006 recommending the use of these tools at well child visits. We offered informal outreach to physicians providing instructions on screening tools, billing information, AAP recommendations and information on referral resources. We quickly recognized that screening alone wasn’t sufficient and began talking about the referral process and how to ensure successful referrals were being made. At around this time, research was showing us that only about 50% of children referred for Early Intervention services were actually connecting to that referral. It was easy to identify children with concerns but not as easy to ensure they received needed support. We decided to try formalizing our approach to outreach by offering Continuing Medical Education [CME] credits. While we didn’t change content, offering CME changed the way providers saw us as detailers. We appreciated the new credibility, but still struggled with recruiting new practices. NaRCAD: Recruiting practices to participate is a challenge for many programs. How did this struggle transform into quality improvement?
We now offer Quality Improvement [QI] and MOC projects for implementing developmental screening, autism screening and postpartum depression screening in addition to a project that aims to increase the percentage of children who successfully connect with Early Intervention when referred from their primary care provider. We have been thrilled with the response from physicians for participating in these projects and just received funding to continue and grow our outreach efforts. NaRCAD: What have been some other challenges you’ve faced when going in to talk to clinicians about implementing developmental screening? Mindy: I started working at ABCD unsure of how to provide physician outreach, so I naturally modeled my efforts on the one successful approach I knew very well, which was pharmaceutical sales. As the recipient of pharmaceutical detailing, it was pretty easy to begin my outreach efforts in a similar fashion. I quickly learned how it feels to be a detailer. Front office staff rejected me repeatedly, I made hundreds of phone calls that didn’t get returned, and when I did get to speak to a provider I had to speak quickly and to the point to keep their attention. The challenge of gaining access was the biggest barrier I confronted early on and remains at the top of the list.
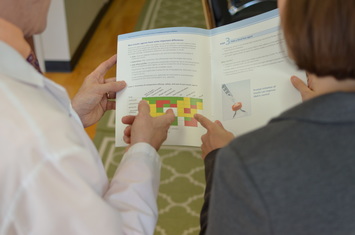 A key challenge: gaining access to clinicians. A key challenge: gaining access to clinicians. NaRCAD: When dealing with those challenges, what’s helped you to build relationships with clinicians in order to gain commitment? Meagan: To deal with the challenges that arise, we have found that it helps to get creative in our approach to gain access to clinicians and add credibility to our messages. A barrier we have encountered when trying to schedule times to meet with clinicians is the expectation that we will provide food. Our funders and budgets do not allow us to pay for food, so we have opted to provide other incentives for clinicians, such as CME or MOC credit. Not only is offering CME/MOC credits an educational incentive for providers, but it lends credibility to our messages. We facilitate our QI projects through multiple meetings at the practice and have found that, by developing relationships and a presence in the office, we can overcome clinicians’ resistance to implementing screening or other changes in their practice.
 Resource and best practices exchange at #NaRCAD2015 Resource and best practices exchange at #NaRCAD2015 NaRCAD: We were happy to see you at our 3rd International Conference on Academic Detailing here in Boston a few months ago. Tell us more about how the conference helped you think about your work in a different way. Mindy: We were thrilled to be able to attend the conference and came away very energized. We highly recommend the conference to anyone doing similar work. Some of our key “take-aways” were around the fundamentals of academic detailing, including the need for profession materials and repeated visits to develop relationships. We came home committed to find money for developing professional materials and to attend the two-day intensive training offered by NaRCAD.
However, I’ve struggled with our role as a non-profit in meeting these needs. Up to this point, ABCD has utilized a very hands-on approach. We plan meetings, take notes, write up PDSA cycles, make “To Do” lists – anything we can do to make the process easy for the practice and allow the providers to concentrate on patient care. A true practice facilitation model is more concerned with increasing the capacity of the practice to continue quality improvement work after the facilitation had ended. The goal isn’t to do all the work, but to help the practice find capacity to do it themselves. NaRCAD: What other advice would give to a new and emerging AD program that’s just getting started, or that you’d give yourself if you could go back in time 10 years? Meagan: We have found NaRCAD’s training and tips to be very helpful, so we would recommend that new clinical educators attend a NaRCAD techniques training to hone their skills in communicating their messages with clinicians and gaining commitment to behavior change. One of our main takeaways from the NaRCAD conference was the importance of high-quality, professional materials, so we would recommend that new programs budget for the development of professional materials as well as food, which can be an incentive when setting up meetings with clinicians. Over the years, we’ve realized how critical it is to work with community partners before going into healthcare practices to ensure that clinical workflows, such as processes for making referrals to external agencies, are aligned with community-defined processes and so that clinicians are aware of the resources available to patients and families in their communities. NaRCAD: Thanks so much for sharing important insights from your program to improve childhood health outcomes. We look forward to seeing you at a future training and hearing more about your program's future successes! BiographiesMindy Craig, PA-C, M.S., Director of Physician Outreach, has been with the ABCD team for 8 years and brings with her experience in the clinical setting. She earned her physician assistant degree at the University of Colorado Health Science Center’s Child Health Associate/Physician Assistant program in May 2000. Concurrently, she completed additional course work and research to earn her Master of Science degree in Pediatrics. Ms. Craig worked as a physician assistant in a number of settings for ten years prior to joining the ABCD team. Her medical career has included a variety of medical office positions from medical records clerk to practice manager. This range of experience positions her to fully understand the unique dynamics and flow in a typical office, which allows her to deliver technical assistance to practices at a meaningful level.
Ms. Craig’s quality improvement experience began in the business sector where she was extensively trained on Total Quality Management (TQM) at Northwest Airlines. She worked at the airline as a facilitator, training inflight and ground personnel in the principles of quality improvement. This experience with quality continued in the clinical setting, as she has participated in and/or chaired a number of quality improvement projects over her career as a physician assistant. In addition to her work at ABCD, Ms. Craig also does consulting work for organizations needing assistance with physician outreach and education. Meagan Shallcross, MPH, Healthy Steps/Physician Outreach Coordinator, joined the ABCD team in June 2015 as the Healthy Steps and Physician Outreach Coordinator. Meagan is passionate about building systems and environments that support children’s healthy development through clinical-community partnerships and integrated care delivery approaches. Meagan earned a Master of Public Health degree at the University of Michigan, where she supported Patient and Family Centered Care projects at the university health system and was involved with community-based participatory research addressing health equity, as well as research focused on provider-patient communication. Learn more at www.coloradoabcd.org. All photos used with permission.
1 Comment
 Trainee Update Series: Where Are They Now? Bevin K. Shagoury, Communications & Education Director Tags: Cancer, Detailing Visits, Practice Facilitation, Training Hi, Emily! We’re happy to reconnect with a NaRCAD trainee, and to feature your current work on this month’s blog. Can you tell us a little about yourself and how you ended up working at the National Colorectal Cancer Roundtable? I’ve worked in public health for 12 years, and in seven of those years I’ve focused on cancer screening and prevention. I got to know NaRCAD while working at the Washington State Department of Health, where I designed their approach and curriculum to coach primary care clinics and health systems on quality improvement strategies to increase colorectal cancer screening. Then last summer I joined the American Cancer Society as the National Colorectal Cancer Roundtable’s new associate director. In this role much of my work is still focused on developing educational resources for providers, but I’m also involved in efforts to increase colorectal cancer screening through other channels, such as public education and policy. I learned so much about effective methods for conducting clinical education from the NaRCAD Academic Detailing training that I participated in back in October 2012. I’m grateful to have the opportunity to reconnect with NaRCAD, and thank you for the opportunity to share an update on my work! Tell us a little bit about background and goals of the Roundtable. The Roundtable, established by the American Cancer Society (ACS) and the Centers for Disease Control and Prevention (CDC) in 1997, is a national coalition dedicated to reducing the incidence of and mortality from colorectal cancer in the U.S., through coordinated leadership, strategic planning, and advocacy. Today, the Roundtable is a collaborative partnership with more than 100 member organizations across the nation. Through the efforts of several task groups, the Roundtable advances initiatives that focus on provider education, public education, health policy, quality and disparities issues. Thanks in part to the work of many of our members, colorectal cancer incidence and mortality rates have dropped by over 30% in the U.S. among adults 50 and older in the last fifteen years, with a substantial fraction of these declines due to screening. Yet, despite the good news, colorectal cancer remains the second-leading cause of cancer death in the U.S. when men and women are combined.  The Roundtable is focusing on a great initiative called “80% by 2018.” What’s the story behind this movement? To accelerate efforts to increase colorectal cancer screening, the Roundtable launched the 80% by 2018 initiative in March of 2014. 80% by 2018 is a movement in which hundreds of organizations have committed to substantially reducing colorectal cancer as a major public health problem and are working toward the shared goal of reaching 80% of adults aged 50 and older screened for colorectal cancer by 2018. To date over 650 organizations – including medical professional societies, academic centers, survivor groups, government agencies, cancer coalitions, cancer centers, payers and many others – have signed a pledge to make this goal a priority. If we can achieve 80% by 2018, 277,000 cases and 203,000 colorectal cancer deaths would be prevented by 2030. You can learn more about 80% by 2018 and pledge your organization’s support on our 80% by 2018 webpage.  A trainee role-plays at a NaRCAD 2-day techniques session. A trainee role-plays at a NaRCAD 2-day techniques session. You attended a NaRCAD Academic Detailing Training a few years back to practice skills in clinical outreach education. Can you tell us a little bit about the highlights of your experience? Academic detailing and practice facilitation are relatively new fields, so when I first accepted a job that included these skills I felt a little in over my head! I was up for the challenge, though, since I saw provider education and training as a way to move further upstream in making substantive and sustainable changes that would positively affect public health. It can take a while for new clinical findings to get implemented in primary care, so I saw that academic detailers and practice facilitators serve a key role in getting these findings into clinical practice. My two-day Academic Detailing Training with NaRCAD taught me practical skills to work in this role, and gave me the confidence to know I could be effective without a clinical background. The highlight was the role-playing and one-on-one feedback from experienced academic detailers. Their personal feedback was not something I could have found in a book or online training. What tools from the training do you think are most relevant to active detailers in the field? Some of the most valuable tools I took from the training were the interpersonal skills needed to be effective as an academic detailer. The tips on how to solicit buy in after sharing a practice change was incredibly useful, such as asking: “does this sound like something you’d be willing to try in your practice?” It was also really helpful to learn how to approach sharing a clinical update that could potentially make a provider feel as though they had been delivering inappropriate care. The training taught me how to navigate these discussions by saying that while something might be common practice it’s no longer supported by the latest clinical evidence. In my experience, providers were very receptive to learning new clinical updates when it was shared in such a way that they did not feel they were being reprimanded for not knowing already knowing the latest evidence. Thanks for chatting with us. We’re happy to help get the word out about “80% by 2018” and looking forward to hearing the results of the initiative. Thank you for the opportunity! I enjoyed reconnecting with you and reflecting on how my training with NaRCAD has enriched my work in clinical education. I’d like to encourage any readers that are interested in 80% by 2018 and efforts to increase colorectal cancer screening to learn about the campaign. And there are lots of great tools and resources in the provider education section of our website that might be of particular interest to academic detailers.  Emily Butler Bell is the Associate Director of the National Colorectal Cancer Roundtable. In this role she manages a number of projects that support the 80% by 2018 initiative, a movement in which hundreds of organizations are working toward the shared goal of reaching 80% of adults aged 50 and older screened for colorectal cancer by 2018. Prior to joining the Roundtable, Emily served as the Cancer Screening Quality Improvement Consultant for the Washington State Department of Health, where she designed their approach and curriculum to coach primary care clinics and health systems on quality improvement strategies to increase colorectal cancer screening.
Prior to that, Emily worked with the American Cancer Society in Austin, TX as a Cancer Information Specialist and later as a Health Insurance Specialist, where she gained insight into the access and affordability issues surrounding colorectal cancer screening. She holds a Master’s in Public Health from Boston University and a B.A. in Psychology from the University of California, Santa Cruz.  Attendees share resources during a networking break. Attendees share resources during a networking break. Bevin K. Shagoury, NaRCAD Communications Tags: Conference, Detailing Visits, Jerry Avorn, Opioid Safety, Practice Facilitation The excitement and breadth of content in this November’s 3rd International Conference on Academic Detailing exceed what we can capture in this blog post. The combination of exciting speakers, engaging panelists, expert breakout session leaders, and national and international attendees eager to problem-solve created a forward-thinking event that inspired all of us working on AD and related outreach educational activities. As you reflect on our event's highlights, we encourage you to access on-demand video, speaker biographies, session descriptions, and more at our Conference Hub resource page.  Dr. Coffin of SFDPH and Dr. Fischer of NaRCAD Dr. Coffin of SFDPH and Dr. Fischer of NaRCAD Kicking Day 1 off and setting the tone for the entire event, NaRCAD Director Dr. Mike Fischer warmly welcomed our packed room at Harvard Medical School’s Martin Center by encouraging collaboration, connection, and sharing. Our Day 1 Keynote Speaker Dr. Carolyn Clancy, the CMO of the Veteran’s Health Administration, described the VHA’s work to improve pain management in the veteran population while addressing the challenges of medication abuse and overdose. Dr. Clancy shared strategy and data behind the national effort and the critical role of academic detailing in it, connecting attendees to a big-picture view that can be adopted to look at other health epidemics and interventions. Our first expert panel presented Practice Facilitation in Primary Care. Andy Ellner moderated the session, leading panelists Ann Lefebvre of North Carolina's AHEC Program, Lyndee Knox of LA Net, and Allyson Gottsman of HealthTeamWorks to discuss strategies, contextualize their work in relation to academic detailing and quality improvement, and share their personal approaches to challenges in primary care behavior change. Allyson Gottsman’s much-appreciated analogy that practice facilitation is not unlike “leading a fisherman to a well-stocked pond” resonated with panelists and participants alike. Many attendees who were actively engaged in practice facilitation in their daily work shared that the panel helped them to think about their work in a new way.  Breakout leaders share a moment during the Day 1 session! Breakout leaders share a moment during the Day 1 session! The afternoon’s breakout sessions offered attendees multiple tracks with AD-related topics to explore: deconstructing and analyzing a 1:1 AD visit, exploring the skills needed to manage an effective AD program, and strategizing on ways to identify and harness stakeholder support when initiating a new program or strengthening an existing one. The afternoon closed with two presentations; the first, by Terryn Naumann of the Canadian Academic Detailing Collaboration (CADC), offered participants a view of the power of synergy and teamwork, the historical context of the CADC’s creation and growth, and the future of the collaboration.  Dr. Avorn gives a presentation one Tweeter called "pure gold" Dr. Avorn gives a presentation one Tweeter called "pure gold" The final presentation of the day was a lively one by NaRCAD’s co-founder and co-director, Dr. Jerry Avorn, who identified major obstacles to effective evidence-based communication in the current landscape of healthcare, and provided a future-centered lens through which attendees could envision how academic detailers can address these challenges. A full day of new ideas and connections culminated in a networking reception that gave attendees a chance to relax and connect socially. Day 2’s morning opened with another engaging Keynote Speaker; Dr. Don Goldmann, CSO & CMO of the Institute for Healthcare Improvement, combined quality improvement theory with personal anecdotes, weaving in real-life examples of successful interventions to provide context and dimension to the theory that underlies all of our work.  L-R Valerie Royal, Joy Leotsakos, Sameer Awsare, Mike Fischer. L-R Valerie Royal, Joy Leotsakos, Sameer Awsare, Mike Fischer. More examples of successful practice change were illustrated by the morning’s Themed Plenary on the Intersection of Public Health and AD. Dr. Phillip Coffin of the San Francisco Department of Public Health shared the success of an intervention focusing on co-prescribing of naloxone to reverse opioid overdose deaths in San Francisco. Another successful AD intervention was presented by Michael Kharfen of the Washington D.C. Department of Health, who highlighted the successful implementation of AD programs to increase HIV and Hepatitis C screening and treatment. The afternoon featured our second Expert Panel, this time on the role of AD within integrated healthcare systems. Moderated by Dr. Mike Fischer of NaRCAD, panelists Joy Leotsakos of Atrius Health (MA), Sameer Awsare of Kaiser Permanente Medical Group (CA), and Valerie Royal of Greenville Health System (SC) shared their experiences using AD in systems at different stages of development. Attendees had the opportunity to discuss this topic further in the afternoon’s breakout sessions, which also included a session on practice facilitation, as well as third session to continue to explore AD and public health partnerships.  Happy to see our colleagues from Norway at #NaRCAD2015! Happy to see our colleagues from Norway at #NaRCAD2015! The conference’s closing discussion was led by Mike Fischer, who thanked not only the speakers, panelists, and session leaders, but the participants, whose willingness to share their experiences within an interactive setting was key in creating solutions to bring back to use in their daily work. The creative collaborations, exchange of resources, excitement in combating challenges in the field, and belief in the importance of AD for the future of healthcare transformation were felt by all at the closing of a very full and thought-provoking event. Our Twitter feed tracks the event’s highlights through #NaRCAD2015, and you can catch our event photo album on our Facebook page. We invite you to explore these topics, learn about our speakers and attendees, and connect with us at the NaRCAD Conference Hub, where you can access on-demand video of all main sessions from the conference. Thank you again to all who attended, and to AHRQ for funding our series. Please stay in touch with us and each other, and continue the conversation and idea sharing below. We hope to see you in 2016!  by Lyndee Knox, PhD Tags: Detailing Visits, Practice Facilitation, Primary Care Practice facilitation is an approach to helping primary care practices improve the quality of care they deliver to patients. Good practice facilitation is practice-centered, meaning that you start where you’re needed and work out from there. One of my favorite stories about the practice-centered nature of facilitation was told to me by Ann LeFebvre, director of the statewide primary care facilitation program in North Carolina. Ann was starting work with a new practice in her community. As is common at the beginning of most improvement efforts, she asked the practice what their greatest concern was at the moment. Ann expected them to tell her they were concerned about improving workflow with their electronic health records, or that they wanted to improve their performance on particular HEDIS (Healthcare Effectiveness Data and Information Set) measures, or that they wanted help engaging their patients more effectively. Instead, what they told her caught her completely by surprise. “We’re really concerned about our patients getting to our practice.” “Oh,” she said, “so you’re worried about access issues?” “Well, sort of,” the staff person responded. “Recently we’ve had a flock of geese take up residence in our parking lot, and they are biting our patients when they get out of their cars to walk inside. Some of our patients are afraid to get out of their cars.” 5 Whys Tool: Click to Learn. As an experienced facilitator, Ann understood how important it was to meet practices where they are at the current moment, not where they “should be.” So she rolled-up her sleeves and said, “Ok, let’s figure this one out.” She saw the problem of the geese as an opportunity to teach practice staff basic principles of quality improvement. She taught them to use the “5 Whys” to determine why the geese were in the parking lot in the first place, and then to use Plan-Do–Study-Act cycles (PDSA) to design and test solutions to the “goose attack” problem. Working together, Ann and the practice discovered that a woman living next door to the practice used to keep and feed the geese. She had recently been hospitalized and because she was no longer there to feed them, the geese had moved into the practice parking lot. Staff developed a solution: to have another neighbor feed the geese – and tested this solution using a PDSA cycle. The geese left the parking lot, their patients no longer had to deal with hungry and aggressive geese in the practice parking lot, and staff had started to build capacity in quality improvement! Practice facilitators are specially trained individuals who work with primary care practices “to make meaningful changes and develop the skills they need to adopt new clinical evidence and health service models in their work and to sustain these changes over time.” (Knox & Brach, 2011; DeWalt, et al., 2010). The primary aim of facilitators, whether working alone or as part of team, is to build practice capacity for continuous quality improvement, as well as to strengthen practice ability to adapt and implement new evidence-based treatments and health service models. Facilitation teams develop long-term relationships with practices. They may work with a practice intensively for 6 to 10 months to implement a specific improvement and then step back for a while. Even though the active facilitation project has ended, they will check-in with the practice every month or two to monitor progress and maintain relationships until they are needed to support another significant improvement project at the practice. While facilitation can be provided by a single individual, (a “practice facilitator”) it is often a “team sport.” The facilitation team is usually led by an individual with expertise in quality improvement processes and methods. This person serves as the team leader and primary point of contact with the practice, and brings in his or her team mates to help the practice as needed. Other members of the facilitation team include individuals with expertise with health IT who can help practices optimize their health IT systems to support the desired changes; team members with expertise in setting up data systems for monitoring performance; and most recently, patient partners. Academic detailers are also essential members of most facilitation teams. They possess deep knowledge about clinical topics and provide 1:1 education to clinicians to increase their knowledge about specific preventive care and treatment issues, encouraging those clinicians to change their behavior to improve patient health. A number of excellent resources are available for training members of facilitation teams, and to guide development of a practice facilitation program. These include the PF Handbook, the National PF Curriculum, and the How to Start and Run a PF Program. Dr. Mike Fischer, the director of NaRCAD, and a team of experts in PF and practice improvement helped develop them. These and other resources that can assist you in building a practice facilitation program in your area can be accessed here. Lyndee Knox, PhD is founding director of LA Net, a primary care practice based research and resource network established with funding from the Agency for Healthcare Research and Quality (AHRQ) in 2002. LA Net supports research and innovation in the healthcare safety net in Los Angeles and provides practice facilitators to practices in its network to support practice-based, clinician and community-led research, evidence translation and practice improvement. Dr. Knox served as principal investigator on AHRQ’s Task Order 13 (TO 13) to examine the use of practice facilitators to implement the Care Model in the safety net, and convened the AHRQ Practice Facilitator Consensus Panel to summarize the state of the field as part of TO13. Most recently she led work for AHRQ to produce a manual to support formation of new practice facilitation programs across the U.S. The resulting manual, Developing and Running a Primary Care Practice Facilitation Program: A How to Guide and case studies are available on AHRQ’s website. As director of LA Net, Lyndee has served as lead on a 2 year contract with the Greater Los Angeles Veterans Administration to create and train a cadre of internal coaches to support its primary care teamlets and PACT transformation. Currently she is working with Mathematica Policy Research to create a 30 module training curriculum for new Practice Facilitators/Coaches for the U.S. AHRQ. Dr. Knox also directs Project ECHO LA, a replication of the successful quality improvement and clinical education intervention from the University of New Mexico aimed at increasing access to specialty care services in rural and underserved areas. Project ECHO LA has been supporting ECHO Knowledge Networks for the LA safety net for 3 years in areas including: psychiatry, preventive care, geriatric medicine and quality improvement. |