The DETAILS BLOG
Capturing Stories from the Field: Reflections, Challenges, & Best Practices

|
An interview with Kelsey Bolton, Continuing Professional Development Consultant, Gundersen Health System by Anna Morgan, RN, BSN, MPH, NaRCAD Program Manager Tags: Detailing Visits, COVID-19, CME, E-Detailing, Smoking Cessation, Substance Use  Anna: Hi, Kelsey! Thanks for taking the time to chat with us today. Can you tell us a bit about your academic detailing program in Wisconsin and your role? Kelsey: I’m a Continuing Professional Development Consultant in the Continuing Medical Education (CME) Department at Gundersen Health System. Gundersen Health System is a teaching hospital with a multitude of specialties that serves patients in Wisconsin, Minnesota, and Iowa. As part of my CME work, academic detailing stood out as an effective tool to disseminate our information and meet our clinicians’ educational needs. We started our detailing program last fall and have been focused on tobacco cessation. The detailing intervention is a spinoff of a performance improvement project we are working on for diabetes. I’m currently a one-woman show; I’m the program coordinator and the sole detailer. I detail physicians, NPs and PAs across the health system. Anna: Wow, it’s incredible that you’ve been able to build your detailing program from the ground up! Can you tell us what that’s been like? Kelsey: Academic detailing was a new concept to me prior to being introduced to it by my former manager, who sent me to the NaRCAD training in May 2019. Academic detailing is not a well-known concept in our hospital system. It was difficult to get past the gatekeepers and “enlighten” them about academic detailing. There are still misconceptions when I walk into a room for a meeting with a clinician – they often think that I’m a drug sales rep, that I’m an internal quality control person, or that I’m there for punitive reasons. I must quickly refute that and explain that I’m there to support and unburden them, not to make judgments about their work. Anna: Those misconceptions are quite common when starting a new academic detailing program. How are you able to “enlighten” the gatekeepers? Kelsey: It was bumpy at first and we tried a few different approaches, but I think we’ve finally been able to smooth it out. I have an advantage because I’m internal and I’m contacting clinicians from an internal email or phone number. I’ve also had our medical program coordinator, the doctor who is partnering with me to learn the clinical information, send out emails to gatekeepers prior to my detailing visits. Anna: Stakeholder buy-in is imperative when building a new detailing program.  Kelsey: Absolutely. Building relationships with key stakeholders has made all the difference. The medical program coordinator I work with, as well as other experts in the organization, helped me curate my detailing aid and key messages. I practiced my detailing sessions with these stakeholders before going out in the field. It was an easy way to build relationships and get them on board – it only took a 15-minute practice detailing session! I’m also fortunate enough to have support from senior leadership. They’ve been able to open doors by letting people throughout the organization know that they support the academic detailing work I’m doing. Anna: It sounds like both managing your academic detailing program and being in the field has helped you be successful in getting your program off the ground. What has it been like to grow and manage your AD program? Kelsey: It’s like herding cats! The detailing program is 25% of my workload, so completing all the administrative work plus the detailing visits is quite a commitment. By the end of this year, I will have detailed over 200 clinicians. “Marathon detailing” has put me in a groove. It has definitely been challenging, but I appreciate that I know the ins and outs of it now – both the administrative tasks and the field work. I feel prepared to help train others. I plan to start training one of my colleagues to become a detailer in the fall. Anna: When thinking about team expansion, it’s also important to think about the impact of COVID-19. How has COVID-19 impacted your program? Kelsey: We paused our detailing visits for about 3 months, and by the time we started talking about bringing them back, NaRCAD was putting out a lot of information about e-Detailing. Before COVID, I had barely done anything with video calling, but getting thrown into working from home, we jumped into a lot of video calls. I learned how to work virtually on the fly, which made it easier to adapt to e-Detailing. I did a few practice e-Detailing sessions with my colleagues and I’ve now successfully completed several visits virtually. The NaRCAD webinars were a lifesaver. We plan to continue e-Detailing until it’s safe to return to in-person visits. Anna: A lot of academic detailing programs had to adapt quickly to e-Detailing during the pandemic. What does the future look like for your program?  Kelsey: For the more near future, we are working on collecting data for the tobacco cessation campaign to eventually publish research on the efficacy of the academic detailing intervention. We’re going to pull patient data from the EMR, as well as look at the qualitative data from the evaluation surveys. This research will help inform our organization on the benefits of academic detailing as an educational intervention. We would also like to continue the program with other strategic initiatives like substance use disorder, social determinants of health, and cancer screening. I have a soft spot for topics similar to tobacco cessation that are sometimes discouraging to clinicians because they don’t feel like they can make a difference. I know that through detailing, I’m able to give them a fresh take on these topics, and reinvigorate them in providing the best care for their patients. Have thoughts on our DETAILS Blog posts? You can head on over to our Discussion Forum to continue the conversation!  Biography. Kelsey Bolton is a Continuing Professional Development Consultant in the CME department at Gundersen Health System in La Crosse, WI and the program lead for its Academic Detailing program. She received her Bachelor of Arts degree in Communication Studies in 2015, Healthcare CPD Certificate in 2019, and is currently pursuing her Master’s in Organizational Leadership. She has completed over 100 detailing visits and is presently conducting a research project on the efficacy of tobacco cessation academic detailing.
2 Comments
NaRCAD's Interview Series: Public Health Detailing Program at New York City Department of Health and Mental Hygiene (DOHMH) Featuring Michelle Dresser, MPH, Senior Manager, Programming & Strategy Tags: Detailing Visits, Diabetes, Evaluation, Obesity, Program Management, Smoking Cessation, Training  Thanks for taking the time to share the great clinical outreach education work that’s being done by the NYC Department of Health and Mental Hygiene, Michelle! Tell us a bit about yourself and how you got involved in public health, specifically public health detailing. Michelle: Thank you for the opportunity to speak about the Public Health Detailing Program. I have over 20 years of public health experience in both the non-profit and government setting, with the last 12 here at the New York City DOHMH. Throughout my professional career, my specialty has been in healthcare marketing and provider education, emphasizing how providers and consumers can better communicate with each other by tailoring complex messages using health literacy principles.
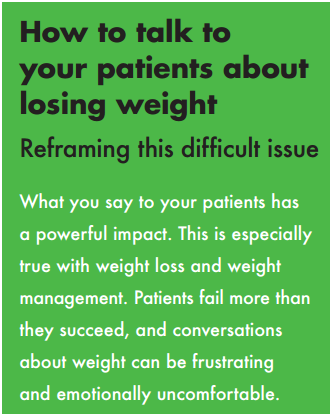 An excerpt from DOHMH's obesity pocket guide. An excerpt from DOHMH's obesity pocket guide. It’s essential our reps have excellent selling and communications skills, so when they engage providers and get their buy-in, providers are then equipped to get their patients “on board”. One-on-one provider engagement helps them understand how important it is to have a 2-way communication with patients. How can an outreach representative encourage providers to “get on board” and think about care as a dialogue? Michelle: Let’s use obesity as an example. With obesity, both providers and patients are frustrated, for different reasons. Providers may be frustrated that patients’ comorbid conditions are being exacerbated or don’t have the same kinds of tools to treat obesity as they do other conditions; patients might feel that providers aren’t using great communication techniques, like motivational interviewing (MI), to help them set goals and take small steps towards the goal. If a patient is only told, “You need to lose weight,” which is such a broad and overarching goal, they’ll be frustrated, and frankly, non-adherent. I know I would be. 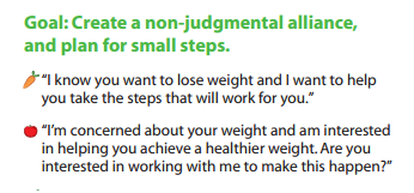 Example of a coaching script created by DOHMH. Click to learn more. Example of a coaching script created by DOHMH. Click to learn more. Encouraging providers to have specific dialogues using a customized approach for each patient is important. This kind of dialogue takes into account patients’ literacy beyond the written and spoken word—it looks at scientific, fundamental, health and cultural literacy, too. We work on “coaching scripts”, which take the key recommendations and reframes them in order to custom-tailor the conversation for each patient.
One thing that’s unique about public health detailing is that we detail the whole team through one-on-one interactions. Evidence shows these types of interactions with providers and staff are more effective at changing behavior; however, sometimes due to the makeup of the practice we must conduct group presentations. It’s not ideal, but it still allows us to get the messages and materials out there.
 A coaching guide designed by the NYC DOHMH to aid clinicians in smoking cessation support for patients. A coaching guide designed by the NYC DOHMH to aid clinicians in smoking cessation support for patients. So when an outreach representative goes into an office, they detail...everyone? Michelle: If there are 15 people who work in an office, we’re going to detail all 15 of them. It’s a lot! Sometimes, the person who is the champion of a new behavior or workflow isn’t going to be the provider. We see the front desk staff as instrumental; they’re interacting with all of the patients. We work with our teams to ensure even the front desk staff receives the materials and information, rather than seeing them merely as a “gatekeeper” to get to the providers. Sounds like a lot of training goes into preparing for your campaigns, and for thinking about the entire process of effective outreach. Tell us more about your trainings, and about how you prepare outreach representatives on disease content training, as well as in marketing and communications skills.  Click to view more Public Health Action Kits (copyright of NYC's DOHMH) Click to view more Public Health Action Kits (copyright of NYC's DOHMH) Michelle: On average, our trainings are about 5 days in length and take place the week prior to launching a new campaign. About 40 percent of the training is disease content, so we work with our internal Health Department experts, as well as external experts, where we learn about prevention strategies, treatment strategies, epidemiology and the landscape around the key recommendations chosen based on the evidence of that topic. We need to know the ‘why’ behind the campaign. Once we have that under our belt, we shift to sessions on how to frame the issue, how to promote the materials, figuring out the “features and benefits” as well as the “barriers and objections” and finally “gaining a commitment”, which are phrases that come from pharmaceutical marketing. We’re “selling” and promoting public health interactions, so we work on those skills. We also do a great deal of role playing, including videotaped analysis of each rep. We look at body language, what communication skills are effective, we do knowledge assessments, quizzes—we make sure our team is well-prepared to go out and detail. We take this seriously—they’re representing the New York Department of Health and Mental Hygiene.
What’s a major barrier your program has faced, and how have you tackled it? Michelle: A big challenge, when starting a detailing program, is access. The landscape of healthcare systems in NYC has drastically changed over the past few years. As an example, several years ago, the majority of our Brooklyn territory was almost entirely made of up of small practices where access wasn’t an issue. What’s changed since then? Michelle: Now, many of these sites have become part of larger institutions, so there’s corporate buy-in that needs to happen for people to come in and talk to the staff. As I mentioned before, although we try and limit group presentations, this has proven to be an effective strategy when entering into a new relationship. Once they get to know us and recognize the value of the program, they’re engaged in having us come back to conduct 1:1 visits on the follow-up and subsequent campaigns. How do you know when a campaign is working and becoming successful? Michelle: Evaluation is always on the top of our priorities, and can be a challenge for any program to evaluate effectiveness. For every campaign we conduct an initial and follow-up visit where we assess provider practice. This allows us to see if there has been a change in practice from the initial to the follow-up visit. Additionally, we rate what providers intend to adopt in terms of the key recommendations and supporting tools and resources. We also collect a large amount of qualitative data because it's also critical to gaining a more complete picture of the campaign’s success, especially when reporting on barriers, access and materials.
You can scale this up or down, depending on your need and organizational priorities. Our program focuses on where there’s the greatest need and potential for greatest impact. Programs should make sure to look at their organization’s agenda and goals. It’s important to look at the data and plan the best course of action within the capacity you have. Biography: Michelle Dresser. Michelle Dresser is the Senior Manager of Programming and Strategy for the Public Health Detailing Program within the Bureau of Chronic Disease Prevention and Tobacco Control at the New York City Department of Health and Mental Hygiene. In this role, she oversees the overall programmatic direction and strategy of the program. This includes, campaign strategy and timing, campaign content, training and economic incentive development, provider selection, identification of targets to ensure the greatest impact on populations most in need, and identification of “new needs” opportunities to expand program reach and achievement of program goals. She also oversees internal and external strategic relationships to enhance programmatic objectives.
An Interview with Mass Mental Health CenterFeaturing Mark Viron, MD, adult psychiatrist & Director of Health Home Services at the Department of Mental Health’s Massachusetts Mental Health Center (MMHC) in Boston; Assistant Professor at Harvard Medical School. Tags: Materials Development, Mental Health, Smoking Cessation, Training NaRCAD: We’re excited to talk about your program because it focuses on such an important population, and such a specific topic that’s been a focus of public health initiatives across the nation. Tell us about Massachusetts Mental Health Center (MMHC). Mark Viron: MMHC is a Department of Mental Health (DMH) community mental health center in Boston that has provided mental health services for over 100 years to people with chronic and persistent mental illness. Its ultimate goal is to help people maintain meaningful and productive lives in their community. In 2013, to better address the significant unmet primary care needs of our patients, we launched the Wellness and Recovery Medicine (WaRM) Center. The WaRM Center offers co-located and integrated wellness and primary care services for all MMHC patients.
NaRCAD: Why, historically, have rates of tobacco use been higher in folks with serious mental illness (SMI)? Why has there been resistance for clinicians to promote tobacco cessation for this group? Mark: It’s a complicated issue. There are risk factors that increase the rate of smoking in this group and these are coupled with obstacles to getting appropriate treatment. People with SMI are overrepresented among populations that face social and environmental conditions that are typically associated with an increased prevalence of smoking – poverty, unemployment, limited education, etc. Obstacles to quitting include limited availability of resources, lack of clinician involvement, and poor social/peer support.
 The strategy of AD: 1:1 clinician-facing outreach. The strategy of AD: 1:1 clinician-facing outreach. NaRCAD: Agreed! What do these AD-focused, 1:1 visits between trained physician educators and psychiatric prescribers entail? Mark: The visits are 20-30 minutes long and follow the typical detailing visit structure. Visits are conducted by me, a psychiatrist at MMHC, or Gail Levine, MD, an internist and the Medical Director of our primary care clinic. We meet with the prescribers in their offices, and begin by asking open-ended questions to assess their needs and learn about their successes (and challenges) in addressing tobacco use with their patients. We celebrate successes and validate challenges, and then pivot to sharing evidence-based information and key messages that may help them address these issues with greater success. We conclude the visit by reviewing steps the prescriber can take to increase successful tobacco treatment, and provide a copy of our detail aid, along with a few high-yield references.  Click to see complete detail aid. Click to see complete detail aid. A key ingredient to our success has been our detail aid. A great psychiatry resident (now attending), Kathryn Zioto, worked with Gail and me and the NaRCAD team to develop a detail aid about tobacco treatment in people with serious mental illness. The detail aid contains cutting-edge, evidence-based information in clear language with colorful graphics. It includes information about the MMHC’S Smoke Free Team, and highlights our three “asks”, which helps clinicians frame their conversations with patients:
NaRCAD: We enjoyed working on this important project with you, and we know how important great materials are in engaging clinicians to consider behavior change. That said, how have psychiatric prescribers been responding? Mark: The response has been quite favorable. It's been rewarding to sit down with colleagues and learn from their experience and expertise and to be able to offer some useful information about tobacco treatment and the Smoke Free Program. The one-on-one detailing encounters, even as brief as they are, give us quality time with our colleagues to focus on their individual concerns and questions. We probably get as much information as we give!
 NaRCAD AD Trainings: hands-on and interactive. NaRCAD AD Trainings: hands-on and interactive. NaRCAD: Two members of your team, yourself and Gail Levine, attended our AD Techniques Training in 2015 to prepare for this initiative. How has the training helped you provide this education to prescribers? Mark: Your training gave us an in-depth immersion into the world of academic detailing, helping us understand theories and evidence and think about implementation issues. Getting to practice detailing and getting feedback from experts in the field was invaluable, as was the ability to talk with people from around the country who are working on similar projects. NaRCAD's training is incredibly worthwhile – it was compact, comprehensive, and helped us acquire the needed skills to implement this project successfully.
 Provider education, engagement and activation are key, and AD provides a framework that has a proven track record in producing results in these areas. Plus, AD is efficient and easily implemented relative to other interventions--especially when you have assistance from NaRCAD! NaRCAD: Thanks for taking the time to connect with us. We’ve enjoyed helping to support this initiative with training and materials development! We look forward to continuing to learn about the impact you have on improving the health of people with serious mental illness, and sharing it with the community. We can't wait to hear more about this intervention at our conference this fall!  Biography. Mark Viron, MD is an adult psychiatrist and Director of Health Home Services at the Department of Mental Health’s Massachusetts Mental Health Center (MMHC) in Boston and an Assistant Professor at Harvard Medical School. He specializes in the treatment of psychotic disorders and the integration of primary and behavioral healthcare for people with serious mental illness.
He graduated from Tulane University School of Medicine and completed his psychiatry residency at the Massachusetts General Hospital/McLean Residency Program. He serves as an attending at MMHC’s partial hospital program, where he teaches and trains residents and medical students. He is also the project director for two grant-funded initiatives that aim to enhance MMHC’s ability to provide integrated primary and behavioral healthcare.  An Interview with Frank Leone on Treating Tobacco Dependence with AD
Dr. Leone directs Penn’s Comprehensive Smoking Treatment Program and was a former trainee with NaRCAD. Tags: Detailing Visits, Smoking Cessation, Substance Use, Training NaRCAD: Tell us a bit about yourself. How did you get into academic detailing? Frank Leone: I’m a pulmonologist, and have been focused on the treatment of tobacco dependence for over 20 years. In my early years, I had always been amazed at how infrequently my colleagues would approach the literature for solutions when facing this common problem in the clinic. It seemed to me that they relied heavily on “common sense” approaches and techniques derived from misunderstandings, rather than consulting published guidelines and available standards. I became interested in the behavioral economics of tobacco treatment decision-making in the clinic, and realized that traditional approaches to changing physician behavior might be inadequate for dealing with a cultural problem this well-entrenched. We initially turned to NaRCAD for advice on Academic Detailing in 2011, and found the approach to have just the right potential to both meet the needs of the target audience, and allow us to deliver our message in a cost-effective and scalable way. We were also given an opportunity to work with the Philadelphia Department of Public Health as they started up their efforts to influence the local provider culture around tobacco, and we’ve been “off to the races” working within our community, creating positive changes, ever since. NaRCAD: What does your program focus on? (What health issue does it address, and what clinician behavior are you seeking to change?) Dr. Leone: Our Academic Detailing (AD) program focuses exclusively on tobacco dependence treatment. As you can imagine, that problem cuts across a number of different audiences. Our detailers work with physicians, psychologists, nurses, counselors and others to impact the rate at which tobacco treatment services are delivered in our area. We use AD to address the limits in knowledge base around pharmacotherapy, as well as to shape the core assumptions about effectiveness of treatment in key patient populations (e.g. those with established lung disease or serious mental illness). NaRCAD: Tell us about some of the growth you’ve seen and been a part of as it relates your program. Dr. Leone: Our AD program has grown every year since its inception. We started out focused on primary care physicians in underserved parts of Philadelphia. From there, we expanded our target audience to include specialist physicians, nurses, and nurse practitioners. Most recently, our audience has expanded to include behavioral health practitioners in both inpatient and outpatient settings. Because of our success using AD to work with care providers from a variety of disciplines, we are currently exploring ways to extend AD principles to “system-wide” approaches to creating behavior change. NaRCAD: What would you say are the greatest challenges you see in implementing this intervention? Dr. Leone: Finding the right people to go into the field is imperative. Over the years, I’ve been impressed that success during the AD interaction is less about what degree a person has, and more about the ability to be gently directive, while willing to truly listen. Detailers need to be spontaneous and responsive to their audience, while at the same time keeping their inner eye on the target. This is a skill that takes a little time and training to develop. It sounds like it ought to be an easy thing to do, but we’ve found that an organized, logical, mentored approach to learning these skills is important to success. NaRCAD: How about what works well? How do you know when you’ve been successful? Dr. Leone: We always try to incorporate some sort of measurement tool into our AD projects. It might be about knowledge, attitudes, or behaviors, but having a metric to gauge our impact is important feedback ensuring we stay on mark. Our funders appreciate a concrete measure of change as well. If I could figure out how to capture this, my favorite measure would measure the “A-ha!” moments that happen so often within the audience. I love the look of epiphany in the clinician’s eye when a detailer has found a way to make the information relevant and transformative. That’s when I know we’re really making change for the long run. NaRCAD: You attended our Academic Detailing Techniques Training a few years back. What are the most useful resources or information that you’re still using today? Dr. Leone: Truthfully, the greatest resource has been the continuing relationship with the NaRCAD team. On multiple occasions during the conception and start-up phases of our project, we were able to touch base with professionals who had a large collective experience in diverse disciplines to get some great tips and suggestions. On one specific occasion, I remember sharing a written detailing piece with the NaRCAD team. We had developed it in hopes of getting some feedback. Not only did we get great advice, but it was professional advice – complete with references, examples, resources, and connections to the theoretical basis for the suggestions. To me, this is the kind of interaction that helps my team grow and learn over time. NaRCAD: What does future success look like for you? Dr. Leone: In twenty years, when you go visit your doctor for your annual check-up, and you hear him or her say, “Of course tobacco dependence is a chronic illness of the brain for which there are a number of effective treatments. It’s hard to believe we used to simply tell people to stop!” –then you’ll know we’ve done our job well. Biography: Dr. Leone received his medical degree from the University of Pittsburgh, School of Medicine, and completed his postgraduate training in both general internal medicine and pulmonary / critical care medicine at Thomas Jefferson University Hospital. He also received his masters degree in clinical epidemiology and biostatistics from the University of Pennsylvania School of Medicine. Dr. Leone directs Penn’s Comprehensive Smoking Treatment Program, a clinical program of the Penn Lung Center, located at both Penn Presbyterian Medical Center, and the Perelman Center for Advanced Medicine. The new program provides state-of-the-art and individualized treatment to smokers, including those with co-morbidities. Dr. Leone’s scholarship focuses on investigating advanced treatment strategies for tobacco use disorder, and on testing educational strategies for improving the care of the tobacco dependant patient. Dr. Leone is a member of several professional and scientific societies, including the Society for Research on Nicotine and Tobacco, the American College of Chest Physicians, and the American Thoracic Society. He has served the Commonwealth of Pennsylvania as a legislative appointee to the Governor’s Tobacco Use Prevention and Cessation Advisory Committee since 2001. Dr. Leone has been invited to speak at numerous lectures on topics of smoking treatment and pulmonary medicine, and has been published in a variety of clinical and research journals. He is board certified in pulmonary and critical care medicine. Learn more and review related publications on the University of Pennsylvania’s site. Read more: Behavioral Economic Insights into Physician Tobacco Treatment Decision-Making : Leone, Frank  Mike Fischer, MD, MS
Tags: Cardiovascular Health, Detailing Visits, Smoking Cessation, Training At NaRCAD, we work together with our many partners, collaborating on important interventions to improve patient health through clinical outreach education. This summer, we’re especially looking forward to a unique collaboration to improve cardiovascular health, as we travel to Oklahoma to support the Healthy Hearts for Oklahoma project, part of AHRQ’s EvidenceNow initiative. EvidenceNow is a group of 7 large studies across the United States working to improve cardiovascular care in small primary care practices. Along with materials development and program support, the NaRCAD team will travel to Oklahoma City in July to train over 20 health professionals, teaching them how to provide the service of academic detailing to participating practices. Focusing on the ‘ABCS’ (aspirin use, blood pressure control, cholesterol management, and smoking cessation), the professionals we train will carry out academic detailing visits in order to present best evidence to participating practices. By using the skills and techniques of AD to assess the needs of clinicians and practices throughout Oklahoma, the detailers we train will gain commitment from clinicians to commit to practice change. The Healthy Hearts for Oklahoma project will visit hundreds of practices, tracking these practices’ behaviors over time. Ultimately, the evidence generated by Healthy Hearts and the other EvidenceNow studies will yield key insights about how best to bring evidence to diverse practice settings and improve the cardiovascular health of all Americans. Supporting organizations that are carrying out important work such as this is at the core of who we are and what we do. The positive impact of academic detailing can be amplified with each new intervention, program, or even a single visit to a clinician. As we enter into our 5th year as the only nationally available resource center for for academic detailing, the strength of the relationships we build makes it possible for clinical outreach education to serve more practices and have a greater impact on patient health. We’ll share highlights from the Healthy Hearts for Oklahoma project and other exciting collaborations with our subscribers this fall. In the meantime, we’d love to see you at a future Boston-based training, or at our 3rd annual International Conference on Academic Detailing this fall—join us as we work together to advance the field of clinical outreach education. |