The DETAILS BLOG
Capturing Stories from the Field: Reflections, Challenges, & Best Practices

|
Anna Morgan-Barsamian, MPH, RN, PMP, Senior Manager, Training & Education, NaRCAD Tags: Stigma, Evidence-Based Medicine, Health Disparities, Conference Missed our event? Check out the AD Summit videos and materials on our Summit Hub.  We’re fresh off of the excitement of hosting our Academic Detailing Virtual Summit, “A Deeper Understanding of Our Impact on Patient Care.” In prioritizing patient-informed care more than ever before, we explored patient narratives through live interviews, workshops, and special panels, all within a virtual space. Innovations included AD for criminal justice involvement, care delivery redesign for veterans, affirming care for transgender and nonbinary people, and patient-informed communication on sex positivity in HIV prevention. Take a peek at some of the highlights from our event below! AD Fireside Chat: A New Spin on a “Keynote Address” We opened our AD Summit with a real-time interview featuring the originator and co-founder of NaRCAD, Dr. Jerry Avorn, and the National Director of the Veterans Affairs Pharmacy Benefits Management Academic Detailing Service, Melissa Christopher. Audience members were excited to throw ideas around and ask questions about:
Program Development Workshops: Attendees Led the Charge! Our revamped course catalog of workshops invited attendees to be in the director’s seat, as well as behind the scenes as co-creators in small groups. Participants created resources that we’ve published on our website and social media channels, sharing creativity and expertise with the larger AD community. Our workshops covered a wide range of topics including:
 The Pleasure Project The Pleasure Project Special Panel: Understanding Critical Care Needed for Formerly Incarcerated Patients The outstanding team from New York City Department of Health and Mental Hygiene (NYCDOHMH) shared their groundbreaking detailing campaign, “Public Health Detailing for Criminal Justice Involvement”, with an audience that was hungry for innovation around inclusivity. The NYCDOHMH team shared NYC clinicians’ understanding of formerly incarcerated patients’ care, including clinicians who met the campaign with stigma, and those who were grateful to see such a campaign being implemented. Best Practices Spotlight: Prioritizing the Patient Experience For the first time in NaRCAD’s history, we highlighted leaders in the field who’ve been prioritizing the patient experience. The San Francisco team created space for conversation and discussion about gender-affirming care and ways to encourage safe clinical environments for transgender and nonbinary individuals through language, storytelling, and community outreach. We also heard from the Arizona team about the importance of pleasure being part of a patient’s sexual health history and the role of a detailer in supporting these conversations between clinicians and patients. 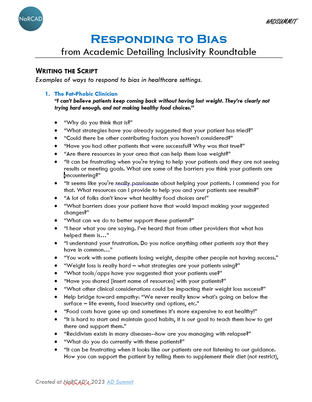 Inclusivity Roundtable: Real-time Script Creation
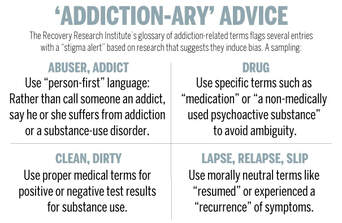
We wrapped up our AD Summit with a roundtable session where attendees co-created a scripting resource to empower detailers to combat stigma during visits. We asked attendees to come up with responses to the stigmatizing comments below. A five-page resource was created in 60 minutes! 1. “I can’t believe patients keep coming back without having lost weight. They’re clearly not trying hard enough, and not making healthy food choices.” 2. “I don’t want those patients at my practice. They’re so difficult to handle and are really just looking for another opioid prescription. Treatment won’t work for them.” 3. “I’m so tired of keeping up with all these different pronouns. You’re either a man or a woman. It gets in the way of providing care.” 4. “I don’t need to use an assessment tool. I can always tell when someone’s at high risk of contracting HIV.” We want to continue these conversations, hear about your team’s innovations, and share resources in person this fall at our annual conference in Boston, MA. We hope to see you there! -The NaRCAD Team A special thank you to all of our AD Summit attendees and presenters as well as our partners at the Agency for Healthcare Research and Quality. For more information on our presenters, you can view the AD Summit Program Book. Have thoughts on our DETAILS Blog posts? You can head on over to our Discussion Forum to continue the conversation! Curated By: Aanchal Gupta, Program Coordinator, NaRCAD Tags: Stigma, Primary Care, Data Time and time again we’ve heard about the challenges detailers face when tackling clinician stigma. Detailers have shared comments from clinicians such as, “We don’t take those types of patients” or “I don’t want to be known as the gay doctor.” Addressing stigma and fostering understanding with clinicians can often feel overwhelming for detailers. In this edition of “AD-vice” we shine a light on these issues and share experiences from our community on how they managed stigma during detailing visits.  Understanding Stigma
 Addressing Stigma through Education and Conversations
 Addressing Stigma through Data and Resources
Our team at NaRCAD is here to learn and support you as we combat stigma and continue to promote inclusivity. Check out our new Healthcare Inclusivity Toolkit for detailers for additional resources.
Best, The NaRCAD Team Tags: Conference, Detailing Visits, Stigma Take a peek at the NaRCAD2022 conference materials on our Conference Hub.  Earlier this month, our team at NaRCAD hosted the 10th annual International Conference on Academic Detailing, “Celebrating 10 Years of Community Engagement.” We hopped on the virtual AD bus and heard from programs from across North America and beyond. This year, the conference featured campaigns focused on menopausal hormone therapy, initiation of antiretroviral treatment (iART), falls prevention, COVID-19, biosimilars, antiracist health care, polypharmacy, and opioids. The theme of community engagement was seen throughout the entire 3-day event, and we’re thankful to everyone who joined from around the world. Check out some of the highlights from our 2022 conference below.  Welcome Addresses:
Field Presentations:
 Breakout Sessions:
Expert Panels:
Special Presentation: “Looking Inward: AD as an Intervention for Antiracist Health Care”:
Real-time Roundtable:
 Thank you for all your engagement and support throughout the last 10 years of NaRCAD annual conferences! We are humbled to see how much the AD community has grown and are excited to be able to feature innovations at our conferences that have informed your work over the years. Our team at NaRCAD will continue to provide space for everyone to come together to share ideas, ask questions, and network. We look forward to seeing you in 2023. -The NaRCAD Team A special thank you to all of our NaRCAD2022 presenters as well as our partners at the Agency for Healthcare Research and Quality! Check out the NaRCAD2022 program book for more information on the presenters. Have thoughts on our DETAILS Blog posts?
You can head on over to our Discussion Forum to continue the conversation!  This series features tried-and-true practices from our AD experts. This week’s guest blogger is Zack Dumont, BSP, ACPR, MSPharm a NaRCAD Facilitator and Academic Detailer at RxFiles Academic Detailing Service. Curated by Anna Morgan-Barsamian, MPH, RN, PMP, Senior Manager, Training & Education, NaRCAD Tags: Detailing Visits, Stigma, Training  Model the compassion you expect from others. In recent years, the academic detailing community has been trying to recognize the harmful role of stigma in many clinical settings and to include stigma reduction in our detailing messages. In applying this framework, we encourage an empathetic view of people who experience stigma. They don’t choose to have addictions, exhibit certain behaviors, or to be ‘villainous’. We can all agree they don’t deserve harsh judgment and criticism. I invite you to bring forth your most charitable mindset for a moment and apply that same framework when you encounter stigma during a detailing visit. Imagine that the clinicians or people you detail hold stigma not because they want to stigmatize others, but for some more relatable reasons: they’re impressionable, they’re naïve, they’re vulnerable. In the same way that a clinician wouldn’t expect someone with a substance use disorder to suddenly recover if harshly confronted, we can’t expect the person who stigmatizes to respond to similar tactics. Be patient, be persistent (after all, you care and want them to be their best selves), and be persuasive with those that you’re detailing. You have a lot of natural talent, training, and experience to efficiently help people make informed decisions through detailing visits. Don’t limit it to therapeutic decision-making; extend it to the mental and emotional aspects of care, as well.  Balance and refine your self-reflections. Alone or with a colleague, find a quick and easy way to debrief after each visit – save the more intense feedback for quarterly or annual reviews. Maybe it’s asking two simple questions like, “What went well?” and “What could have gone better?” and taking a moment to reflect on each. And, just like AD visits which are 90% prep and 10% execution, the more the better when it comes to ‘prepping’ your self-reflection questions. So, “What went well?” could be more specific to one of your strengths:
Your “What could have gone better?” question could focus on an area of improvement unique to you:
This isn’t easy, but it’s low risk with the potential for big reward… so I encourage you to jump in! Want more tips? Stay tuned for the next installment in our Words of AD Wisdom series, and reach out to the NaRCAD team, subscribe to our network, or check out our discussion forum to hear more tips and ways to train your brain!  Biography. Zack is a clinical pharmacist with the RxFiles Academic Detailing Service in Regina, Saskatchewan, Canada and an expert facilitator for NaRCAD's training courses. He has been involved with the RxFiles since 2008, with experience in both academic detailing and content development of RxFiles’ evidence-based drug therapy comparison tools. Zack also serves as the Clinical Manager for the Saskatchewan Health Authority Pharmacy Department. His practice has largely been hospital-based, with more specialized experience in anticoagulation and heart failure. His professional interests include evidence-based medicine, information technology, and leadership.
Zack graduated as a Pharmacist from the University of Saskatchewan in 2008. Following graduation, he completed a hospital pharmacy residency with the Regina Qu’Appelle Health Region. He also completed a Master’s degree in Pharmacy, with a focus on leadership, from the University of Cincinnati. By Anna Morgan-Barsamian, MPH, RN, PMP, Senior Manager, Training & Education, NaRCAD An interview with Lexie Hach, Regional Health Specialist, Bureau of HIV, STD, and Hepatitis, Capacity Extension Program, Iowa Department of Public Health. Tags: Detailing Visits, Evidence-Based Medicine, Stigma, Rural AD Program  Anna: Hi, Lexie! We’re excited to chat with you today about your detailing work in rural Iowa. Your program started about 5 years ago and was born out of the HIV and Hepatitis Community Planning Group (CPG). Can you share more about the CPG and how the detailing program was created? Lexie: The CPG is made up of healthcare providers, people with lived experience, case managers, educators, and other stakeholders. The group serves in an advisory capacity to the Bureau of HIV, STD, and Hepatitis at the Iowa Department of Public Health (IDPH) and their main task is to ensure that the state has an inclusive participatory planning and evaluation process for the delivery of prevention and care services. About 5 years ago, the CPG recognized a need for more education in the rural parts of Iowa related to best practices in HIV, sexually transmitted infections (STIs), and Hepatitis. That’s when we learned about AD. We started building our detailing program based on a lot of the work that New York City’s program was doing. We now have 5 detailers, who we call Regional Health Specialists (RHS).  Anna: What an interesting start to your program! You’re currently assigned to detail in 15 counties in central Iowa covering over 20 sexual health topics, from stigma to your statewide condom program to new screening recommendations. Do you detail on these topics beyond the primary care setting? Lexie: Yes! Our goal as detailers is to provide the best health outcomes for people living with HIV and those living with, or at risk for, STIs and Hepatitis C. We meet with the medical community including, local health departments, community-based corrections, substance use specialties, mental health, and many community based organizations. We also attend a variety of community meetings. We know that many people living with HIV pass through community-based organizations. We want to make sure that those organizations are equipped with the correct information to get people the care they need through resources or referrals. Our team has created detailing materials for both medical professionals and community-based organizations to maximize our impact. Anna: Working with community-based organizations is a great way to make sure people have access to the best possible prevention and care, especially in a rural state like Iowa. How does Iowa’s geography impact your detailing work?  Lexie: Iowa has 3.1 million people with about 54 people per square mile. Our state is 85% farmland with country roads, winter weather, and a lot of construction. It is not uncommon to lose cell service or your GPS signal while driving in the very rural parts of Iowa. We’ve adapted our detailing approach because of this and have found that group sessions work best for us. We identify champions in the clinics and are then able to set up 1:1 visits with clinicians as needed. Anna: We often hear from programs that group detailing is a great way to get your foot in the door and spread the word about AD. It’s nice to know that it’s working so well for your program too! I imagine Iowa’s geography also impacts patient care. Lexie: Yes, it does. There can be stigma around seeking sexual health care in rural parts of Iowa. Many times, patients know someone working at the clinic in their town. It’s common for patients to travel long distances to get to a clinic where they don’t know anyone. It’s also common for patients to have to travel over 2 hours to access HIV care at a specialty clinic. Anna: And that’s 2 hours one way! Has your program been able help with increasing access to care? Lexie: Yes, I can share one story that stands out the most to me. A couple of years ago, I was presenting at a community meeting with 15 or so people in attendance. The CEO of a federally qualified health center (FQHC) in Southern Iowa was also present and we were able to connect and network afterwards. We talked about how far patients must travel for Ryan White HIV care and he saw a need that the community health center could fill. We connected with senior leadership, there were additional meetings, and together we were able to bring Ryan White HIV care services to the health center. Those services are still there today and now people living with HIV in Southern Iowa can access Ryan White services closer to home. Anna: There is so much to be said about the power of AD, networking, and champions! Let’s wrap up with hearing about some of your program’s successes from this past year. Lexie: We’re so proud of all that we’ve accomplished this year! Here are some highlights: 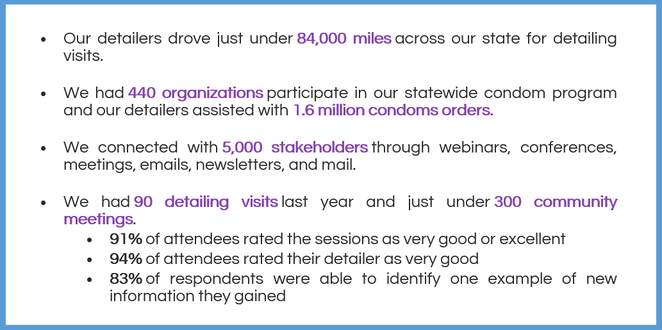 Anna: Those are some impressive numbers across both the clinical and community settings. Thank you for letting us feature your detailing work and learn more about the impact your team is making in your state! Have thoughts on our DETAILS Blog posts? You can head on over to our Discussion Forum to continue the conversation!  Biography. Lexie Hach holds an Associate Degree in Nursing, Bachelor of Arts degree in Health Promotion and Women’s Health, and a Master of Arts degree in Community Health Education. Lexie is currently a Doctoral student in Public Health (DrPH) with an Epidemiology concentration at the University of Nebraska Medical Center (UNMC).
Lexie has held positions in nursing, health education, public health, and healthcare marketing. Lexie has been with the Bureau of HIV, STD, and Hepatitis Capacity Extension Program at the Iowa Department of Public Health for over five years as a Regional Health Specialist (RHS). Lexie was previously with the bureau as a Disease Intervention Specialist (DIS). Lexie was instrumental in developing and implementing the RHS program in Iowa’s rural communities. In her RHS (academic detailing) role, Lexie educated a variety of different stakeholders on best practices related to HIV, STIs, and Hepatitis in central Iowa. Lexie has helped support the Sexually Transmitted Disease (STD) Program as a DIS due to COVID-19 and also helped as a COVID-19 contact tracer. Lexie was the previous workforce health department co-chair for Iowa’s statewide strategic plan to stop HIV in Iowa (Stop HIV Iowa). Lexie recently returned to her roots in the STD program and now serves as an Integrated DIS and Special Projects Coordinator, but continues to work alongside her fellow RHS colleagues. By Anna Morgan-Barsamian, MPH, RN, PMP, Senior Manager, Training & Education, NaRCAD An interview with Trish Rawn, BScPhm, PharmD, Clinical Service Director and Academic Detailer, Centre for Effective Practice (CEP). CEP is a not-for-profit in Canada that aims to close the gap between evidence and practice for healthcare providers. Tags: Stigma, Detailing Visits, Substance Use  CEP's COVID-19 Resource Centre CEP's COVID-19 Resource Centre Anna: Hi Trish! Thanks for joining us today. Your team has been working on a number of AD campaigns including, falls prevention, type 2 diabetes, benzodiazepine use in older adults, chronic non-cancer pain (CNCP), and opioid use disorder (OUD). Can you tell us about some of the other recent work you’ve been doing at CEP? Trish: Our team’s academic detailing work is a big part of what we do, but CEP has other supports as well. We create clinical tools and resources on myriad clinical topics where practice gaps have been identified. Our most popular resource has been our COVID-19 Resource Centre to support primary care clinicians in adapting their practice during the pandemic. It’s become a massive resource that has had over 140,000 downloads. Anna: Wow! That’s an impressive amount of downloads. One of the other priority areas where your team has identified practice gaps is OUD. This topic often has a lot of stigma associated with it. Is this something you’ve experienced with the opioid detailing campaigns?  Trish: When we first started detailing on CNCP, opioid tapering, and OUD, there was a lot of fear and stigma among clinicians. They didn’t want to be known as the doctor “prescribing all the opioids.” Some clinicians were concerned that they might get in trouble, and they’d say things like, “I don’t have any of those patients” or “They’re all inherited patients.” Clinicians also sometimes felt like they didn’t want to say the wrong thing to patients, so they wouldn’t say anything at all. We’re all guilty of this and we’ve tried to encourage language like, “Hey, I might be saying the wrong thing here, but let's just start the conversation.” Anna: Just starting the conversation with the right intentions is helpful, even if you don’t get the language completely correct. Have you seen any stigma at the patient level? Trish: We found that patients themselves were experiencing stigma when seeking help and when trying to talk openly about opioids with their clinicians. Family doctors are in a vital position to help patients because they tend to have long-term, trusting relationships with them; they have sometimes taken care of them since they were children. Studies show that when opioid replacement therapy is prescribed by family doctors, there are improvements in patient uptake, patient satisfaction, and treatment success. We wanted to get the clinicians to a place where they felt confident talking with patients about opioids and where their patients felt comfortable sharing their experiences. It may feel like a jump for a clinician to go from, “I'm here to measure your blood pressure and adjust your medications” to “Let's talk about opioid addiction and set goals around tapering.”  CEP's Opioid Use Disorder Tool CEP's Opioid Use Disorder Tool Anna: I can see how talking about OUD might make some clinicians feel uncomfortable. What types of resources has your team developed to support both clinicians and their patients to feel more comfortable having these conversations? Trish: For our academic detailing visits on opioids and CNCP we developed a resource called Talking Points with Patients, which includes scripts for clinicians to handle different scenarios. For example, one of the scenarios is about a patient asking for a dose increase for an opioid, but the clinician not agreeing that a dose increase will help manage their pain. We also have a Specific, Measurable, Achievable, Relevant, and Time-Bound (SMART) Goals resource to help clinicians set goals with their patients by taking the focus off the pain number scale and focusing on actions like, “What activities would you like to do if you had less pain?” Anna: It’s clear that your team works hard to develop and tailor resources to support clinicians and patients. What kinds of local resources from your community are available for detailers to share with clinicians? Trish: We often help clinicians find local resources through a program called The Healthline, which is a website that connects patients with social supports, like counseling, food, and safety. We’re also lucky to have Rapid Access Addiction Medicine (RAAM) clinics in our community that are a one-stop shop for patients with OUD where they’re assessed, given support and a plan for tapering, and referred to other community services. Anna: It’s so important for clinicians and patients to be linked to local resources and know that they have a community supporting them. Can you share some data about how clinicians reacted to the opioid-specific campaigns overall?  Trish: Absolutely! I can share some key findings from our opioid campaigns. Opioid therapy for CNCP AD campaign (n=475): After the detailing sessions, clinicians indicated they were confident in their ability to have a conversation about tapering when appropriate, even when the discussion was challenging (93.5%). Non-pharmacological and non-opioid alternatives for CNCP AD campaign (n=323): Clinicians indicated that after the detailing sessions they were confident in their ability to help patients:
OUD AD campaign (n=250): Clinicians indicated that the detailing sessions enabled them to support patients with OUD by:
Anna: That’s incredible. It’s obvious that your campaigns have made a huge impact on clinicians. What advice would you give to other AD programs who are supporting clinicians in reducing stigma, especially as it relates to opioids? Trish: I would recommend remembering three key points: Examine your own biases: When developing detailing tools, you need to make sure that you’re aware of your own biases and that your tools include the lens of equity, diversity, and inclusion. This is something we are actively working on incorporating in all our work at CEP. Make space for clinician experiences: It’s important to remember to be sensitive to the clinician perspective. There have been times, especially with opioids, where clinicians have had painful experiences with patients overdosing. Be aware of their perceptions and respectful of the trauma they may have experienced. Know your patient population: Understand who the patients are, the trauma they’ve faced, and the stigma they may endure. Look at the experiences of your team, the clinicians, and the patients you’re working with and try to understand how these different perspectives all influence one another as you develop your resources. Anna: That’s beautifully said, Trish. Thank you so much for sharing about your important work in reducing stigma around OUD. Have thoughts on our DETAILS Blog posts? You can head on over to our Discussion Forum to continue the conversation!  Biography. Trish Rawn is the Clinical Service Director for the Centre for Effective Practice Academic Detailing Service. She is a hospital pharmacist who has been detailing for 6 years on topics such as antipsychotics in the elderly, opioid tapering, chronic pain, diabetes, falls prevention, and benzodiazepine deprescribing.
Aanchal Gupta, NaRCAD Program Coordinator Tags: Conference, Detailing Visits, Stigma, E Detailing, Opioid Safety Take a peek at the NaRCAD2021 conference materials on our Conference Hub.  Fresh from our move to Boston Medical Center, our team at NaRCAD hosted the 9th annual International Conference on Academic Detailing, a virtual event concentrating on “Cultivating Relationships for Community Resilience.” There were robust discussions on critical topics, useful tools shared, and connections built. With over 300 registrants from across the globe, the AD community continues to learn and grow thanks to your support and passion for this work. Check out some of the highlights from our 2021 conference below. Day 1 + 2 Welcome Addresses
Field Presentations
Breakout Sessions
Expert Panels
Special Presentation: “Detailer Training in Action: Ask the Experts”
Real-time Roundtable
  Our team at NaRCAD is immensely grateful for your continued feedback and insights during our conference. This community has a wealth of knowledge to share, and as we approach 2022, we plan to continue to facilitate opportunities to connect you with others in the field, create a space to have conversations about stigma, and support your needs in the field. We look forward to seeing you in 2022. -The NaRCAD Team A special thank you to all of our NaRCAD2021 presenters! |
 | Elisabeth Fowlie Mock, MD, MPH, FAAFP is a self-employed Family Physician consultant living in Holden, Maine. She attended Vanderbilt Medical School and obtained a Master’s in Public Health at UNC-Chapel Hill. She is a clinical educator for the Maine state Academic Detailing program (MICIS) and Alosa Health in Boston. She is Board Certified in both Family Medicine and Addiction Medicine. Her part-time clinical work includes evening shifts as a hospitalist and prescribing at a high-risk, low-barrier buprenorphine clinic. She is passionate about women’s and girls’ basketball, travel, learning chess and singing. |
 Dr. Mizroch participating in a NaRCAD training
Dr. Mizroch participating in a NaRCAD training 








4/30/2019
 Don Teater role playing at an academic detailing training in Ware County, GA
Don Teater role playing at an academic detailing training in Ware County, GA 
 Source: Harvard Gazette
Source: Harvard Gazette 

 Image from UNAIDS
Image from UNAIDS 
 Image: University of New Mexico
Image: University of New Mexico 
10/26/2018

|
"I would tell new detailers to take a deep breath and know that you’re ready for this. NaRCAD does such a good job of training us as detailers, and you just feel ready." -Carol Furlong, Academic Detailer |
What have been some of the best visits you‘ve had when you’ve met with clinicians 1:1?
Carol: A rewarding moment for me was hosting a small dinner for any staff member interested in hearing about MAT, because nine people from across the organization attended! There was a level of excitement that was really amazing, and everyone who attended left the dinner ready to get waivered, and to get their friends involved too. Other than that, I’ve had really memorable exchanges with clinicians who start out skeptical, but then become very open and grateful when they discover that my primary goal is to listen to them and their needs. They can be dumbstruck that I truly want to help them, and to find them the resources for them to be successful. |