The DETAILS BLOG
Capturing Stories from the Field: Reflections, Challenges, & Best Practices

The Impact of Childhood Experiences on Patient Health: AD to Encourage Trauma-Informed Care1/31/2022
By Anna Morgan-Barsamian, MPH, RN, PMP, Senior Manager, Training & Education, NaRCAD  As we’ve jumped right into 2022 programming, our team at NaRCAD continues to support detailing efforts that improve outcomes for vulnerable populations, recognizing that patient needs are complex and often informed by social determinants of health. One critical topic for which we’ve developed resources focuses on detailing to improve patient health as informed by both adverse and positive childhood experiences. We’re seeing an increased need from our community members to support detailing efforts related to this critical topic. We partnered with the National Association of County and City Health Officials (NACCHO), Centers for Disease Control and Prevention (CDC), and consultants from Brigham and Women’s Hospital and Tufts Medical Center over the past two years to develop academic detailing materials for clinicians working with both adults and children. The CDC defines adverse childhood experiences (ACEs) as traumatic events that occur in childhood, including abuse, neglect, and family dysfunction. These events are linked to poor health outcomes in adulthood like chronic health problems, mental health conditions, and substance use. When considering the impact of environment on health, the CDC notes that children are likely to flourish when they have safe, nurturing relationships. These supportive settings create the opportunity for positive childhood experiences (PCEs). PCEs can mitigate the effects of ACEs and toxic stress, promote healing from traumatic events, and foster healthy development and learning in children.  Encouraging clinicians to consider both ACEs and PCEs is a natural fit for clinical outreach educators. There are many reasons that clinicians may not be prepared to have conversations with patients about childhood experiences. Perhaps the clinician doesn’t have a behavioral health provider to consult within their practice, so they don’t know who to turn to if a patient discloses a traumatic experience. A detailer can encourage a clinician to explore this concern, as well as provide a list of local behavioral health providers in the community. Another barrier may be that clinicians could feel hesitant to approach discussions related to trauma, or may not have the skills to do so with sensitivity. In this case, detailers can offer tools that illustrate supportive language that creates a safe environment for patients to share their experiences. Supporting clinicians in using evidence-based tools to build trust with their patients signals that it’s not only okay to talk to patients about this sensitive topic; it’s vital for clinicians to lead these conversations in order to ascertain their patients’ needs and promote patient-centered decision making. A detailer can encourage clinicians to adopt new behaviors through specific key messages, including asking clinicians to take the following steps to support adult patients:
 When clinicians are supporting pediatric patients, detailers can deliver this set of evidence-based key messages, encouraging clinicians to:
 With evidence-based tools, successful AD interventions related to ACEs can result in multi-faceted support for patients, such as stronger connections with community resources, mental health supports, and more trusting relationships between clinicians and their patients. We hope to continue to explore this important and complex topic together as a community. If your program is currently working on an ACEs or PCEs AD campaign, or is interested in starting one, please reach out to us so we can support the development of your programming. We always love collaborating and learning more about the important work that you’re doing, and we hope to continue to build our resources and create toolkits in support of complex topics such as these that intersect with other behavioral health and prevention-focused AD campaigns. Have thoughts on our DETAILS Blog posts?
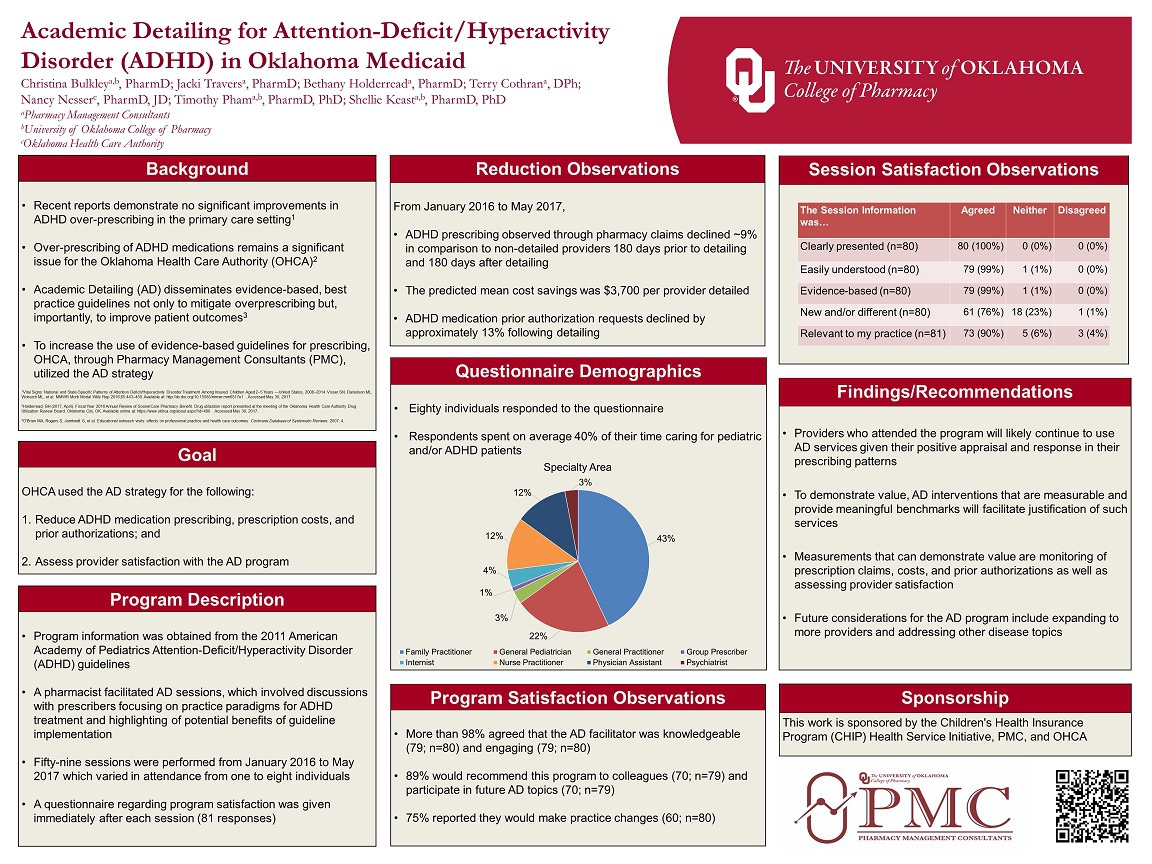
You can head on over to our Discussion Forum to continue the conversation! A ROADMAP for Detailing Success: Improved Outcomes for the Medicaid Population in Oklahoma12/7/2018 Guest Blogger: Jacki Travers, PharmD Clinical Academic Detailing Pharmacist Pharmacy Management Consultants NaRCAD Training Alumnus Tags: Detailing Visits, Mental Health, Pediatrics In June of 2015, I had never even heard the term “academic detailing.” If you’d asked me to define it, I might have said it had something to do with the relationship between teachers and their cars. Little did I know that I was about to become an academic detailer, embarking on an exciting, rewarding, and sweaty-palmed journey to bring evidence-based materials to providers across the state of Oklahoma.
The Oklahoma Medicaid population is mostly under age 21. Detailing topics have included treatment of ADHD, use of atypical antipsychotic medications, and decreasing the use of antibiotics for treatment of upper respiratory infections. We are a small program by comparison, having one full-time detailer since 2015. We added one quarter-time detailer within the last year.  I will share some specific activities that worked for us, which creates a ROADMAP that has served us well and may help you as you begin or enhance your detailing efforts. R – Review When each set of materials neared completion, we asked the experienced NaRCAD staff to review our materials. Having an outside source helped clarify any confusion and identify ways to help the AD visit flow more naturally. O – Objectivity In identifying providers, we were making a bit of a judgement about their prescribing. As a detailer, I found it unhelpful to bring these judgements into the detailing visit. It is important for providers to see detailers as an ally for change rather than a source of punishment or criticism. A – Acceptance We surveyed providers’ acceptance of the program with each AD visit by asking them to evaluate the detailer and the materials. We also asked if they were willing to participate in future visits and recommend the program to colleagues. D – Define Defining the expected care gaps helped guide creation of our key messages. The treatment guidelines for ADHD are well established and remain unchanged since 2011. Comparing these guidelines to national and state patterns gave us a starting point for developing key messages. In addition to published guidelines, evaluation measures such as the Healthcare Data and Information Set (HEDIS) were very helpful. Doing this examination on the front end helped us begin with the end in mind and ensured we collected data we needed from the start. M – Motivational Interviewing Motivational interviewing (MI) is a communication style that is used to modify behavior. MI techniques helped us avoid some of the pitfalls that can accompany potentially confrontational conversations. A – Appealing Graphics We use Adobe Creative Cloud, which we find it to be very user-friendly. For someone with no graphic design experience, YouTube training videos were very helpful. We also use Pixabay as a source for ready-made graphics. All materials are open source and royalty free. We looked at the graphics used by other programs and even materials distributed by pharmaceutical representatives. Having appealing graphics is necessary for any AD program. P – People Having professional mentoring has helped move our program to the next level. Specifically, our detailers received invaluable preparation from the excellent NaRCAD Training Series. Moreover, I never miss the chance to learn from all the presenters and breakout participants at the International Conference each year. We are encouraged by the outcomes we have seen to date. The ADHD campaign produced a 58.33% reduction in medication claims for the very young (age 0-4) and cost savings of more than $226,000 across all ages. The antipsychotic campaign produced a 19.51% reduction in medication claims across all ages with associated savings of more than $365,000. I hope this snapshot of our program demonstrates that even small AD programs can show sizeable improvements in health outcomes and improve utilization of healthcare resources. Now, more than three years later, my understanding of academic detailing is much deeper and continues to grow with each new challenge. I was not completely wrong in my definition though: I absolutely see myself as a teacher and I certainly spend a lot of time in the car!
 Tags: Autism, CME, Conference, Detailing Visits, Pediatrics, Practice Facilitation, Training NaRCAD: Hi, Meagan and Mindy—thanks for taking the time to talk with us about your clinical outreach education programming at Colorado ABCD. Can you give us an overview about ABCD and its mission to improve child development? Meagan Shallcross: Colorado Assuring Better Child Health & Development (ABCD) works with community partners, pediatric healthcare providers, early learning providers, and families across Colorado communities. The goal is to strengthen systems and identify children with developmental delays, connecting them with community services as early as possible.
 Meagan Shallcross, MPH Meagan Shallcross, MPH NaRCAD: Tell us a bit about your backgrounds. How did you each get into healthcare improvement? Meagan: My background in public health, along with experience working in clinical settings and behavioral science research, developed my interest in healthcare improvement that aims to bridge community work and clinical practice, standardize clinical workflows, and ultimately improve experiences and outcomes for patients and families  Mindy Craig, PA-C, M.S. Mindy Craig, PA-C, M.S. Mindy Craig: My path to healthcare improvement is a little different than what you might expect. I worked for Northwest Airlines as a flight attendant for several years straight out of college. At that time the airline industry was losing a large amount of money and needed to find a new way of operating. They decided to utilize a Total Quality Management approach and enlisted people from every department to undergo training in TQM and then facilitate small departmental groups in quality efforts. It was through this process that I began to understand the importance of doing business with a quality framework.  Learn more at coloradoabcd.org. Learn more at coloradoabcd.org. Eventually, I left Northwest and started working in a Neurology clinic while going back to school with the goal of becoming a PA. After completing my degree I worked in primary care settings for about 10 years. I participated in small clinic QI efforts over the years and continued to be interested in quality improvement. I was hired by ABCD 8 years ago to bring a clinical perspective to their physician outreach. It was a natural progression for me to start approaching our work at ABCD with a quality improvement framework. The power of engaging front line staff to implement changes that result in improvement remains as strong as it was when I worked in the airline industry. NaRCAD: Talk with us about your academic detailing programming at ABCD—you’ve been doing this for about 10 years, right? Mindy: We started our work encouraging the use of standardized developmental screening tools in the primary care settings. This was supported by the American Academy of Pediatrics policy statement in 2006 recommending the use of these tools at well child visits. We offered informal outreach to physicians providing instructions on screening tools, billing information, AAP recommendations and information on referral resources. We quickly recognized that screening alone wasn’t sufficient and began talking about the referral process and how to ensure successful referrals were being made. At around this time, research was showing us that only about 50% of children referred for Early Intervention services were actually connecting to that referral. It was easy to identify children with concerns but not as easy to ensure they received needed support. We decided to try formalizing our approach to outreach by offering Continuing Medical Education [CME] credits. While we didn’t change content, offering CME changed the way providers saw us as detailers. We appreciated the new credibility, but still struggled with recruiting new practices. NaRCAD: Recruiting practices to participate is a challenge for many programs. How did this struggle transform into quality improvement?
We now offer Quality Improvement [QI] and MOC projects for implementing developmental screening, autism screening and postpartum depression screening in addition to a project that aims to increase the percentage of children who successfully connect with Early Intervention when referred from their primary care provider. We have been thrilled with the response from physicians for participating in these projects and just received funding to continue and grow our outreach efforts. NaRCAD: What have been some other challenges you’ve faced when going in to talk to clinicians about implementing developmental screening? Mindy: I started working at ABCD unsure of how to provide physician outreach, so I naturally modeled my efforts on the one successful approach I knew very well, which was pharmaceutical sales. As the recipient of pharmaceutical detailing, it was pretty easy to begin my outreach efforts in a similar fashion. I quickly learned how it feels to be a detailer. Front office staff rejected me repeatedly, I made hundreds of phone calls that didn’t get returned, and when I did get to speak to a provider I had to speak quickly and to the point to keep their attention. The challenge of gaining access was the biggest barrier I confronted early on and remains at the top of the list.
 A key challenge: gaining access to clinicians. A key challenge: gaining access to clinicians. NaRCAD: When dealing with those challenges, what’s helped you to build relationships with clinicians in order to gain commitment? Meagan: To deal with the challenges that arise, we have found that it helps to get creative in our approach to gain access to clinicians and add credibility to our messages. A barrier we have encountered when trying to schedule times to meet with clinicians is the expectation that we will provide food. Our funders and budgets do not allow us to pay for food, so we have opted to provide other incentives for clinicians, such as CME or MOC credit. Not only is offering CME/MOC credits an educational incentive for providers, but it lends credibility to our messages. We facilitate our QI projects through multiple meetings at the practice and have found that, by developing relationships and a presence in the office, we can overcome clinicians’ resistance to implementing screening or other changes in their practice.
 Resource and best practices exchange at #NaRCAD2015 Resource and best practices exchange at #NaRCAD2015 NaRCAD: We were happy to see you at our 3rd International Conference on Academic Detailing here in Boston a few months ago. Tell us more about how the conference helped you think about your work in a different way. Mindy: We were thrilled to be able to attend the conference and came away very energized. We highly recommend the conference to anyone doing similar work. Some of our key “take-aways” were around the fundamentals of academic detailing, including the need for profession materials and repeated visits to develop relationships. We came home committed to find money for developing professional materials and to attend the two-day intensive training offered by NaRCAD.
However, I’ve struggled with our role as a non-profit in meeting these needs. Up to this point, ABCD has utilized a very hands-on approach. We plan meetings, take notes, write up PDSA cycles, make “To Do” lists – anything we can do to make the process easy for the practice and allow the providers to concentrate on patient care. A true practice facilitation model is more concerned with increasing the capacity of the practice to continue quality improvement work after the facilitation had ended. The goal isn’t to do all the work, but to help the practice find capacity to do it themselves. NaRCAD: What other advice would give to a new and emerging AD program that’s just getting started, or that you’d give yourself if you could go back in time 10 years? Meagan: We have found NaRCAD’s training and tips to be very helpful, so we would recommend that new clinical educators attend a NaRCAD techniques training to hone their skills in communicating their messages with clinicians and gaining commitment to behavior change. One of our main takeaways from the NaRCAD conference was the importance of high-quality, professional materials, so we would recommend that new programs budget for the development of professional materials as well as food, which can be an incentive when setting up meetings with clinicians. Over the years, we’ve realized how critical it is to work with community partners before going into healthcare practices to ensure that clinical workflows, such as processes for making referrals to external agencies, are aligned with community-defined processes and so that clinicians are aware of the resources available to patients and families in their communities. NaRCAD: Thanks so much for sharing important insights from your program to improve childhood health outcomes. We look forward to seeing you at a future training and hearing more about your program's future successes! BiographiesMindy Craig, PA-C, M.S., Director of Physician Outreach, has been with the ABCD team for 8 years and brings with her experience in the clinical setting. She earned her physician assistant degree at the University of Colorado Health Science Center’s Child Health Associate/Physician Assistant program in May 2000. Concurrently, she completed additional course work and research to earn her Master of Science degree in Pediatrics. Ms. Craig worked as a physician assistant in a number of settings for ten years prior to joining the ABCD team. Her medical career has included a variety of medical office positions from medical records clerk to practice manager. This range of experience positions her to fully understand the unique dynamics and flow in a typical office, which allows her to deliver technical assistance to practices at a meaningful level.
Ms. Craig’s quality improvement experience began in the business sector where she was extensively trained on Total Quality Management (TQM) at Northwest Airlines. She worked at the airline as a facilitator, training inflight and ground personnel in the principles of quality improvement. This experience with quality continued in the clinical setting, as she has participated in and/or chaired a number of quality improvement projects over her career as a physician assistant. In addition to her work at ABCD, Ms. Craig also does consulting work for organizations needing assistance with physician outreach and education. Meagan Shallcross, MPH, Healthy Steps/Physician Outreach Coordinator, joined the ABCD team in June 2015 as the Healthy Steps and Physician Outreach Coordinator. Meagan is passionate about building systems and environments that support children’s healthy development through clinical-community partnerships and integrated care delivery approaches. Meagan earned a Master of Public Health degree at the University of Michigan, where she supported Patient and Family Centered Care projects at the university health system and was involved with community-based participatory research addressing health equity, as well as research focused on provider-patient communication. Learn more at www.coloradoabcd.org. All photos used with permission. |


{kind=link}