The DETAILS BLOG
Capturing Stories from the Field: Reflections, Challenges, & Best Practices

|
An Interview with Lutricia Woods, RN OVERVIEW: Bell County, Kentucky was one of 4 original sites selected for years 1 + 2 of a pilot program of the CDC (Centers for Disease Control and Prevention), NACCHO (the National Association of County and City Health Officials), and our team at NaRCAD (The National Resource Center for Academic Detailing). This exciting pilot program focused on community-level work with local public health departments to develop customized interventions to reduce opioid overdose and death. Six sites experiencing significant public health problems related to opioids were selected over the two years to be trained in academic detailing; those trained health professionals then conducted 1:1 field visits with front line clinicians to impact behavior around prescribing, treatment referrals, and patient care, all within a rural area. As year 2 comes to a close, we’re showcasing stories from the field. Tags: Detailing Visits, LOOPR, Opioid Safety, Rural AD Programs, Substance Use  NaRCAD: Hi Lutricia, thanks so much for taking the time to speak with us about your work as an academic detailer for the opioid crisis in your community. Can you talk to us about how the opioid crisis has presented itself in Bell County, Kentucky? Lutricia: There’s not a family in this community that hasn’t been touched by the opioid crisis in some way. Twenty years ago, I worked in hospitals as an RN discharging patients and providing them with their prescriptions as they prepared to go home. At the time, I was shocked at the rates of prescriptions of opioids with benzodiazepines, and patients thinking it was safe. From my perspective, in our community, the opioid crisis really began by doctors beginning to prescribe many opioids to their patients without education or an understanding of the dangers. Three years ago, I was working on a project at a middle school, and was surprised by the number of grandparents that were raising their grandchildren because their children were either in jail, or otherwise affected by opioid use disorder [OUD]. In Bell County, we also have so many people unable to find a job because they cannot pass a drug test, and once that happens, they return to use because of the stressors of not being able to find a job and pay their bills, and it becomes a challenging cycle to overcome.  NaRCAD: Thanks for sharing your perspective, Lutricia—it can be true that some clinicians don’t see the impact of their role in prescribing opioids, and many times may believe that people who develop an opioid use disorder do so because of a moral failing, rather than seeing it as a medical issue. Did you think 1:1 outreach, provided directly to prescribing clinicians, would lend itself to improving patient health in response to the opioid crisis in this community? Lutricia: I desperately hoped it would. The opioid crisis is very personal to me, as it is to many people in our community. Years ago, my mom had 2 surgeries within 6 months. She had complications from one of those surgeries, and as a result, she was in the hospital for 6 weeks, during which time her care providers did not wean her off of the opioids she took immediately after the surgery. She returned home with prescriptions for opioids at a high dosage, and she developed opioid use disorder. My mother’s doctor, with whom I worked, reached out to have a conversation with me. He told me that I had to be the one to intervene with my mother because she continued requesting more opioids. I conveyed that I wanted her to discontinue taking them, and that he needed to assist us in finding a way to do this, as I felt his prescribing without discussing safety caused the initial issue. His response was that he wanted to “keep her happy.” My mother struggled for the rest of her life; she was able to completely wean off and discontinue using them, but it required a lot of counseling. As a result of this experience, I became a drug education coordinator, as I really wanted to do my part to mend the opioid crisis by providing drug education for every student in the county. And then, of course, I became an academic detailer for this project over the course of the past 2 years, which involves clinician education about safety and risk of opioid prescribing.  NaRCAD: Thank you for sharing that Lutricia; the opioid crisis is personal to so many of us. What would you say has been the most impactful piece of this academic detailing intervention as you went into the field and spoke with clinicians? Lutricia: The most impactful piece has been the ways in which we’re trying to hold clinicians accountable for their roles in the crisis, as well as leveraging their ability to improve things based on their relationships with their patients. For many of the doctors and nurses I met with, our conversations and educational resources have made them more thoughtful and intentional about their role. They seem to realize more that they have the power to decrease the number of prescriptions they write, the length of time for which they write them, and talk more with their patients about safety. NaRCAD: That’s fantastic. What about the most challenging part of this project—what’s been hardest about meeting with clinicians to talk about the opioid crisis in Bell County? Lutricia: Getting an appointment to go in and meet with these clinicians has been so frustrating and challenging. I always say that the receptionists in doctors’ offices are the most powerful people in the world. If you can’t get through them, you’re not going to get what you need, and it is the same with the patients. I couldn’t even get in to see my husband’s doctor, who we’ve known since we were kids. My husband had an appointment, so I resorted to going with him, and did a detailing visit on the spot with his doctor. This same doctor ended up changing practices, and it’s been a lot easier to get into that practice—all because of the office manager. Those relationships are important.  NaRCAD: Getting in the door is definitely a consistent challenge across many programs. We’ve heard from other detailers that practice makes perfect, and sometimes it’s easier to gain access when you actually show up and request a meeting in person. What else did you learn after being in the field?
Lutricia: When I was “volun-told” that I would be attending a training, and doing “academic detailing”, I didn’t truly understand what it was or what the impact would be. I’m a big picture person, and I couldn’t see the big picture at all; I went into that training not knowing what to expect. It wasn’t until I actually started making visits that I could start to see the seeds we were planting to begin to have an impact. Share your thoughts on this piece in the comments section below, or learn more about the LOOPR project and other opioid safety academic detailing initiatives here and on our Detailing Directory.
0 Comments
Guest Blog Interview: David O’Riordan, MPharm, MPH, PhD Senior Pharmacovigilance Officer Pharmaceutical Care Research Group University College Cork, Ireland Tags: Detailer Visits, International, Training NaRCAD: Thanks for speaking with us, David! Tell us a bit about your professional background in healthcare, and how you became involved in academic detailing. David: I am a pharmacist by training, and a couple years ago I decided to carry out a PhD in Clinical Pharmacy at the University College Cork. As part of the PhD, I completed a systematic review examining how pharmacists can be utilized to optimize prescribing in primary care, including through academic detailing. After finding NaRCAD’s resources through a Google search, I registered for the NaRCAD conference in Boston. Dr. Fischer, Dr. Avorn, and all the other attendees at the conference were very encouraging. I left the conference determined and enthused to lead an academic detailing intervention back home. Dr. Avorn and Dr. Fisher put me in touch with Eimir Hurley, a PhD scholar in Ireland, who formerly worked in academic detailing at Alosa Health, and who ended up being a great help in executing the intervention.  NaRCAD: That’s terrific—it sounds like you had a great team at your disposal to begin this work. Can you tell us a little about the unique characteristics of the Irish health system? David: Ireland has a public and private health system. Public patients are more likely to wait longer for appointments. Private insurance is a substantial cost to individuals, though. The health care system is quite fractured unless you’re a private patient. Pharmaceutical drug representatives are also allowed to visit primary health practices here. NaRCAD: In April, you published a study titled “Pharmacist-led academic detailing intervention in primary care: a mixed methods feasibility study” in the International Journal of Clinical Pharmacy. Why did you choose urinary incontinence as a clinical topic? David: As this was a feasibility study, I decided to use one topic as part of the intervention. I organized a meeting with a group of general practitioners (physicians) who would be involved in the academic detailing intervention. The topic of urinary incontinence was chosen by the physicians because they highlighted that it was a topic not discussed regularly among themselves, and currently their only source of information is provided by pharmaceutical drug representatives.  NaRCAD: What barriers to success did you come across in your feasibility study? David: For this project, I was the only academic detailer. I started detailing after going to the two-day Basics Academic Detailing Training in Boston in May 2016. In some cases, during the roll out of the intervention I found it difficult to get past the practice manager, but luckily I had learned strategies on getting in the door in Boston that were useful in my effort. On a few occasions, the practice managers didn’t follow through on connecting me with the physicians. I got around this by utilizing physicians I knew in other practices to gain access to their practice. A lot of it came down to how well you know the physicians. I was lucky that they trusted me when I spoke to them. When I did get to meet with physicians, they all seemed very enthusiastic. NaRCAD: Can you talk a bit more about how receptive physicians were to academic detailing? David: Absolutely! This was a mixed methods study, so my colleague Eimir Hurley carried out focus groups after my detailing sessions to evaluate the feasibility of the intervention. Eimir conducted the focus groups on my behalf to reduce bias. The physicians liked that I wasn’t from a pharmaceutical company and that the sessions only lasted 10-15 minutes. They liked that local physicians had chosen the topic, and I wasn’t coming with my own agenda. NaRCAD: How are you or others going to use your feasibility study results to implement across the country? David: I am currently not involved in academic detailing, but I hope to be again in the future. If someone from another part of Ireland read my paper, they would recognize that physicians are very willing to take part in academic detailing. From my experience physicians didn’t feel threatened and really enjoyed the interaction. They liked the interactive style of the visits, and the way that that the evidence was delivered. My study provides a platform for other researchers to detail to a wider group of physicians in Ireland. NaRCAD: Anything else? David: I am very grateful for the NaRCAD team for providing the academic detailing training. I knew literally nothing about academic detailing, and through meeting their team members Sarah Ball, Amanda Kennedy, Mary Liz Doyle-Tadduni, and others, I felt encouraged to go back and detail. I was the only person from Ireland at the training, and the NaRCAD team gave me some useful feedback. I really enjoyed academic detailing, and I was especially proud when my paper was published. I discovered there is an appetite for this educational intervention in Ireland.  Biography
David O’Riordan, MPharm, MPH, PhD Senior Pharmacovigilance Officer Pharmaceutical Care Research Group University College Cork, Ireland David holds a Masters in Pharmacy (MPharm), Masters in Public Health (MPH), Post Graduate Certificate in Teaching and Learning in Higher Education (PG Cert) and a PhD in Clinical Pharmacy. He has extensive experience as a community pharmacist. He previously worked as a Lecturer in Clinical Pharmacy in University College Cork (UCC). While there, he contributed to and assisted in the delivery of research-led teaching at undergraduate and postgraduate level. He also supervised on a number of research projects. He was a clinical trials pharmacist involved in the Thyroid Hormone Replacement for Subclinical Hypo-Thyroidism Trial (TRUST). This was a randomised placebo controlled clinical trial comparing levothyroxine to placebo in community dwelling older adults (≥65 years) with subclinical hypothyroidism (SCH). He is also a tutor on the Irish Pharmacy Union (IPU) Academy. This educational initiative was developed by the IPU to support pharmacist engagement with Continuous Professional Development (CPD). He is currently the Senior Pharmacovigilance Officer at the HRB-Clinical Research Facility, UCC.  Tags: Detailing Visits, Stigma As we reflect on the two major public health topics we’ve been focusing on as we’ve traveled to public health departments across the United States, we’re learning that the public health detailers we’ve been training are discussing much more than just evidence with the clinicians they’re meeting. When we train new health educators on the methods of interactive, 1:1 education, we’re asked most often to customize our curriculum to cover two of the most highly stigmatized topics today: the opioid crisis, and HIV prevention. As the topic of stigma has come up at every straining we’ve implemented this year, our training team has added dedicated time to our trainings to discuss ways to address clinician stigma that arises during 1:1 detailing visits. So, what, exactly, is stigma? It’s defined as “a mark of shame or discredit,” and appears in numerous ways, including through labeling, stereotyping, discrimination, and social inclusion. One of the biggest myths about stigma is that some people carry it, and some people don’t. However, stigma is not binary, and we all possess the ability to stigmatize another group that we perceive to be an ‘outsider’ group. Historically, stigma has appeared mainly in the form of social inclusion, with those identified as ‘others’ being treated as societal outcasts. The interactive approach of AD is well-suited to address clinician stigma by creating a space in which the detailer can ask the kinds of needs assessment questions that can identify the source of these stigmatizing perspectives. When a 1:1 visit is facilitated by a skilled clinical outreach educator who is curious about clinicians’ experiences and genuinely wants to help implement sustainable change, many clinicians feel comfortable in sharing beliefs, identifying patterns, and building relationships based on trust and service. Our language and beliefs will continue to evolve as we continue to learn, encourage one another, and be empathic. We can do this by holding each other accountable in a non-punitive way, pairing our best intentions with education to use inclusive, supportive language, and committing to holding one another accountable by identifying moments when we witness stigma, in order to correct, reflect, and move forward. We’ve seen the potential for change; the medical community’s understanding of substance use disorder and HIV prevention has improved significantly over the past few decades. Outside of our training settings, where else can we start? We’d very much like to hear from you, our community members, about how you’ve experienced or witnessed stigmatizing behavior as it has occurred within the healthcare setting. If you’re an outreach educator, tell us about a time you’ve seen stigma arise from a clinician’s perspective, and what you thought was behind it. If you’re a patient or a provider, talk to us about ways in which you’ve experienced or carried stigma. Keeping a dialogue open and encouraging sharing is one of many steps towards a connected medical community that embraces its patients, clinicians, educators, and supporters with compassion, clarity, and support.
Thanks for reading, and please share your thoughts and experiences in the comments section below! The NaRCAD Team Moving Beyond Skepticism: Partnerships to Improve Health Outcomes in St. Francois County, Missouri7/24/2019 An Interview with Amber Elliot, BSN, RN, Assistant Director, St. Francois County Health Center St. Francois County, Missouri was one of two sites selected for year 2 of a pilot program of the CDC (Centers for Disease Control and Prevention), NACCHO (the National Association of County and City Health Officials), and NaRCAD (The National Resource Center for Academic Detailing). This exciting pilot program focused on community-level work with local public health departments to develop customized interventions to reduce opioid overdose and death. Six sites experiencing significant public health problems related to opioids were selected over the two years to be trained in academic detailing; those trained health professionals then conducted 1:1 field visits with front line clinicians to impact behavior around prescribing, treatment referrals, and patient care, all within a rural area. As year 2 comes to a close, we’re showcasing stories from the field. Tags: LOOPR, Opioid Safety, Program Management, Rural AD Programs 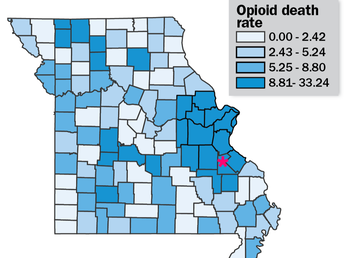 Bureau of Vital Statistics, Missouri Department of Health and Senior Services Bureau of Vital Statistics, Missouri Department of Health and Senior Services NaRCAD: Thanks for joining us to talk about academic detailing in St. Francois, Amber. Let’s start the conversation with some background information about your county. How has the opioid crisis presented itself in your community? Amber: As with many other places, St. Francois County has certainly felt the impact from the opioid crisis. We have high rates of overdoses and over-prescribing. There have also been more children in foster homes because their parents have an opioid use disorder, as well as increasing drug arrest rates. Many aspects of our community have been affected in some way or another. I think this is the main reason why so many community agencies have come together to start working on this issue.  NaRCAD: Why did you think the strategy of academic detailing would lend itself to improving patient health in response to the opioid crisis in your community? Amber: Academic detailing is a great strategy to reach out directly to clinicians in their offices in order to provide resources and supportive education without punitive actions. We really weren’t sure what to expect with having two nurse practitioners, two registered nurses, and a pharmacist carrying out the 1:1 detailing visits. Health Center administration and detailers were skeptical of how physicians would react to other disciplines “telling them how to do their job”. However, academic detailing isn’t telling them what to do, it’s talking with them about what they can do to keep their patients safe. It is a partnership. Missouri is the only state without a statewide PDMP. St. Francois County passed an ordinance to join the St. Louis County voluntary PDMP in 2017. The first report from the PDMP showed St. Francois County as the highest prescribing county in the state. This was a big concern for the Local Board of Health and, we learned from community partners, the citizens of St. Francois County. Health Center administration has presented opioid-related health data for the county at various meeting and kept hearing from partners that clinician outreach education and patient education were top priorities when it came to prescription opioids.  NaRCAD: So, it sounds like it’s been a success so far. What would you say has been the most impactful piece of this intervention? Amber: The greatest success of academic detailing in St. Francois County so far has been the willingness of most physicians to start the conversation about how they can improve prescribing patterns, and care of patients at risk for or experiencing opioid use disorder (OUD). Also, many physicians have started using the PDMP regularly as a result of our academic detailing visits. NaRCAD: That’s excellent news and shows the impact that 1:1 education can have! Over the course of this pilot project these past 4 months, what has the greatest challenge been with implementing a successful academic detailing intervention to improve opioid safety in St. Francois? Amber: The challenge are the providers who do not want to talk with the detailers, or the ones who flat out refuse to change their prescribing patterns. As a nurse, this is frustrating to me because I believe in quality, evidence-based healthcare for all. The refusal to learn, or seek to learn, new information about medications that are prescribed daily is poor patient care and our citizens deserve better than that.  NaRCAD: That does sound frustrating! During our 2-day training, we really emphasis the importance of asking open-ended questions to draw clinicians out. However, there will always be some clinicians who will not engage, no matter how great of a detailer you are. Victoria Adewumi from the original cohort of LOOPR detailers discussed that in a prior blog post. What is something you wish you knew prior to joining the LOOPR Academic Detailing project? Amber: I wish I’d known more about choosing detailers. Recruitment is important. When recruiting detailers, it is more important to make sure to recruit people who have the bandwidth to do the detailing, rather than making sure they have the perfect clinical background. It may be a good idea to create a formalized agreement to ensure they completed their required detailing visits. NaRCAD: You are spot on, Amber. Recruitment is a complex process. Readers can learn more about this later in the summer when we release our new Implementation Guide to help sites like yours select and hire the right candidates. Readers can read other LOOPR blog interviews here, and stay plugged in for more LOOPR site highlights in the next couple of months.  Biography
Amber Elliot, BSN, RN Assistant Director St. Francois County Health Center Amber Elliott is the Assistant Director for the St. Francois County Health Center in Park Hills, MO. She received her Associates Degree in Nursing in 2008 from Mineral Area College to become a Registered Nurse. She went on to obtain her Bachelor’s Degree in Nursing in 2011 from Central Methodist University. She has spent most of her nursing career working in acute settings, primarily hemodialysis. Amber started working in public health four years ago in hopes to make her own community a healthier, safer place to live. Amber has been working on opioid-related activities since 2017. She currently resides in Farmington, MO with her husband and two children.  Tags: Conference, Training Summer's officially here, and we're excited for what lies ahead in public health, especially when it comes to what clinicians can do to improve their patients' health. Here at NaRCAD, our work encourages front line care providers to think differently when it comes to opioid safety, sexual health and STI prevention, cancer control, reducing overmedication for the elderly, and much more. For health educators who provide 1:1 outreach to clinicians, NaRCAD provides hands-on, intensive training, so that these educators can make an impact when bringing the best evidence to front line staff. If you haven't been to one of our trainings, we've just opened registration for our September 23 & 24th, 2019 session here in Boston, where you'll spend 2 days with us, learning how to effectively and persuasively communicate with doctors, nurses, and pharmacists, helping them to increase the chances that their patients will have better health outcomes.  Space fills up fast, so register today, and join other health professionals from across the US who are looking to strengthen clinician care in their communities. After the training, you can bring the interactive interpersonal communications skills of academic detailing back to your health system or local health department to roll out interventions to support chronic disease management, substance use disorder, HIV prevention, and many other critical clinical topics. And if you're already in the field doing this important outreach work with providers, we want to hear from you, and feature you on the DETAILS Blog. Better yet, join us this November 7 & 8, 2019 at our 7th Annual International Conference on Academic Detailing and share your work with our community. Meet others who are advancing the field, infusing clinical care with the best evidence-based tools and approaches in health care.  Want to hear from our community members? And keep your eye on our Twitter feed, and check our News & Media Center for our latest e-news and CoRE Podcasts, or browse the DETAILS archives to the right for more stories from the field.
For our part, we'll be adding new stories this summer on successes and challenges in implementing academic detailing in partnership with our colleagues at CDC and NACCHO to support patients dealing with opioid use disorder and pain management. and we'll be hitting the road to train new detailers in Kansas this August. Stay tuned! Happy Summer! The Team @ NaRCAD Share your work in public health with us. What's happening in your community around the opioid crisis? HIV prevention? Patient education? Have an idea you'd like to hear more about on our next Podcast? Want to share new ideas or challenges related to public health detailing? Sound off below. Building a Team to Improve Local Vaccination Rates: Strategies to get your "Foot in the Door”5/2/2019 Featuring: Kimberly C. McKeirnan, PharmD, BCACP Director of the Center for Pharmacy Practice Research, Washington State University College of Pharmacy and Pharmaceutical Sciences Tags: Detailing Visits, Program Management, Vaccinations  As a pharmacist, I spend a lot of time teaching. I teach patients how to take their medications, how to choose over-the-counter products, and how to identify whether or not to treat minor ailments at home, in the pharmacy, or by seeking care from a physician. I also get to teach other health care providers when one of the medications they prescribe to a patient will interact with the patient’s other medications or cause side effects that will be problematic. After teaching informally in the pharmacy since 2005 and more formally as a Clinical Assistant Professor for the College of Pharmacy and Pharmaceutical Sciences at Washington State University since 2013, my transition to become an academic detailer was natural.  In 2014 I teamed up with an interprofessional group of colleagues to apply for grant funding to improve the low pneumococcal immunization rates in our local rural areas. Our project proposed utilizing academic detailing to teach healthcare providers about pneumococcal immunizations and the importance of immunizing patients. The CDC Advisory Committee on Immunization Practices (ACIP) released a recommendation to vaccinate all patients 65 and older with the new PCV-13 pneumonia vaccine in combination with the longstanding PPSV23 vaccine as part of a two-dose series. Having two pneumococcal vaccines with a complicated vaccination schedule has been challenging for providers. I often hear the questions from my colleagues: “Why are there two, do we really need two?”, “Which one do I give first?”, “When do I give the second one?”, and “What if I give them too close together, do they still work?” Additionally, during a needs assessment of our area we found that many rural pharmacies in our area do not vaccinate at all or only stock certain vaccines because they don’t want to cause competition with the local physicians. We were successfully funded with an Independent Grant for Pfizer’s Learning and Change from Pfizer in 2015. During the first phase of the project, we attended the NaRCAD training program in 2015. The NaRCAD training provided a solid foundation for the framework of our project.  However, once we started talking to local providers about coming in to provide academic detailing, we ran into a major barrier. Getting our “foot in the door” with local providers was harder than we expected. It became clear that our team would need to expand to include more healthcare providers and that we would need to focus our efforts on convincing local medical clinics and pharmacies to invite us in to detail their teams. We expanded our team to include two pharmacists, one nurse, two physicians, two student pharmacists, one student nurse, two medical students, and on biomedical data analysis student. Our team physicians were able to identify physician champions and convince local medical practitioners that our detailing would be helpful for the medical team. They conveyed the message that we weren’t trying to rearrange things – just offer support the clinics. Four pharmacies and two medical clinics invited us to provide detailing.  For the medical clinic visits, we were able to give 15-minute presentations during staff meetings at each location. Attendees included hospital administrators, practitioners, pharmacy staff, nurses, medical assistants, and front end office staff. We appreciated the opportunity to reach so many disciplines at once since immunizations can be recommended by several different health disciplines and at several points during an office visit or hospitalization. Our detailing visits were so well received that we were asked to come back to one of the medical clinics to provide a more in-depth educational program to all of the nursing staff. The second clinic invited us back to meet with hospital leadership to discuss specific points where interventions could be implemented, such as using an EHR alert, putting up signs, or simply asking patients if they were interested in receiving an immunization. We identified several clinical pearls for teams that are considering getting into academic detailing:
McKeirnan KC, Colorafi KJ, Panther SG, Potyk D, McCarthy J. Teaching the Healthcare Team about Pneumococcal Vaccination Practices for Older Adults through Academic Detailing. The Senior Care Pharmacist. Accepted March 2019, in press.  Biography
Kimberly C. McKeirnan, PharmD, BCACP Director, Center for Pharmacy Practice Research, Washington State University College of Pharmacy and Pharmaceutical Sciences Kimberly C. McKeirnan, PharmD, BCACP, is a Clinical Assistant Professor in the Department of Pharmacotherapy at the Washington State University College of Pharmacy and Pharmaceutical Sciences. Dr. McKeirnan graduated with her Doctor of Pharmacy degree from WSU in 2008 and joined the faculty at WSU in 2013 after five years in community pharmacy practice. She is the Director of the newly developed Center for Pharmacy Practice Research at WSU and enjoys teaching student pharmacists about patient care and research. Dr. McKeirnan is passionate about research involving community pharmacy, public health, and improving patient access to quality care services. Dr. McKeirnan has received grants for improving immunization rates in rural areas, developing a model for implementing chronic disease-state management services in rural community pharmacies, and developing a pharmacy technician immunization training program. Optimism for the Opioid Crisis: Addressing Stigma and Disseminating Evidence to Clinicians4/30/2019 An Interview with Don Teater, MD, MPH, Founder, Teater Health Solutions by Kayland Arrington, MPH, Program Manager at NaRCAD Tags: Opioid Safety, Stigma  Don Teater role playing at an academic detailing training in Ware County, GA Don Teater role playing at an academic detailing training in Ware County, GA NaRCAD: Can you tell us about your background? How did you become an addiction treatment specialist? Don: I was trained as a primary care physician, and my wife, Martha, is a behavioral health specialist. The two of us had an integrated-care model, where we did a lot of addiction treatment. I wanted to address that more specifically. An important part of my practice has always been to help those who couldn’t otherwise get help. I did medical work in Honduras, and then I realized that we had a large population of migrant farm workers where I lived in North Carolina. Most of these farm workers didn’t speak English or have a way to receive healthcare. With the help of others, I then opened a free clinic. As far as addiction, I realized that so many patients initially became addicted from my colleagues and me prescribing opioids. The opioid crisis is a public health issue, and medical school doesn’t train you for public health work. Medical thinking addresses what is going on right now, but public health is so much bigger than that. I decided to get a master of public health degree at the University of North Carolina, and I completed that in 2017.  NaRCAD: How does Academic Detailing lend itself to the opioid crisis? Don: Academic detailing can help by having more people with lived-experience do the detailing. In Wisconsin, people with lived experience are either going out with a detailer as a team or doing the detailing themselves. There is also a shortage of people treating OUD. AD is a great program for sharing how to get waiver trained to prescribe buprenorphine for OUD. AD lends itself well to the opioid crisis because it’s an area where little changes can make a big impact. 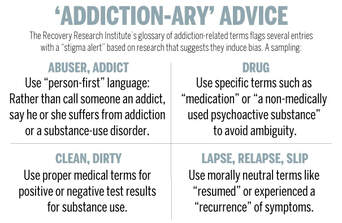 Source: Harvard Gazette Source: Harvard Gazette NaRCAD: There is a huge problem with stigma when it comes to opioid use disorder (OUD), as with any substance use disorder. How can we combat stigma? Don: I hear a lot from other clinicians that they don’t want “those people in my waiting room.” They are picturing someone who is all strung out on heroin on the street corner. We don’t get any education on addiction in medical school and the whole concept is overwhelming to clinicians. The best way to overcome stigma is for clinicians to have interactions with more people with OUD. I think that can be done by clinicians prescribing buprenorphine. I had to deal with my own stigma. For example, I had patients on opioids for chronic pain. I then found out they got arrested or were getting drugs from somewhere else, and I would just fire them from my practice. I saw them as bad people. Once I got trained to prescribe buprenorphine, I listened to their stories. I had made the same choices as many of my patients, yet they became addicted because of their personal history, social history, and genetics. There’s also the importance of language. A lot of the older language around OUD identifies with bad choices and bad people. For example, relapse is associated with a fault of the person. When we are talking about a person with OUD, we are talking about someone with a disease and relapse is a natural course of the disease. When a patient’s blood sugar goes up, we don’t call it a relapse. Just like people with diabetes, we will never cure a person with OUD, but we help them manage.  NaRCAD: We have heard from detailers that many clinicians ask "isn't medication-assisted treatment (MAT) just trading one drug for another?" What do you say to that? Don: There is so much data that shows the first and best treatment for OUD is MAT. There are 11 criteria for OUD, and they are all behavioral. Once people get on the medication, they meet zero of the criteria for OUD. We don’t have many medications for other diseases that can do that. France had a big problem with heroin, and by making buprenorphine more readily available, overdose rates dropped by 80% in 2 years.  NaRCAD: Based on all your research and knowledge, what can be done to stop the opioid crisis? Don: We need to prescribe fewer opioids. A lot of our medical education is still driven by pharmaceutical companies. AD can help by disseminating the evidence on the appropriate treatment of pain. It was only in 2016 that the CDC first came out with guidelines saying opioids should not be the first line of treatment for people with chronic pain. It typically takes 17 years for research to become routine care, and there has already been a lot of uptake with this. Next, we should have all clinicians prescribing buprenorphine, like what France did. We also need to change our criminal justice system to reduce penalties for being found with a controlled substance, including heroin. I am optimistic about each of these things, and think they are all likely to be done in our lifetime – hopefully in the near future.  Biography
Don Teater, MD, MPH Founder Teater Health Solutions Don Teater is a family physician who has lived and worked in western North Carolina since 1988. His work in the southern Appalachian Mountains made him aware of the problems with opioid pain medications years ago. In 2004 he started a clinic to treat those addicted to opioids in his primary care practice. From 2013 to mid-2016, he worked as Medical Advisor at the National Safety Council addressing the national epidemic of opioid abuse, addiction, and overdose. Dr. Teater was lead facilitator for the expert panel discussion during the development of the CDC Guideline for Prescribing Opioids for Chronic Pain — United States, 2016. Dr. Teater has also served on the World Health Organization Committee addressing drugged driving that met in Mallorca Spain in December 2015. Since June 2016, Teater has worked for Teater Health Solutions to concentrate on educating prescribers and others on the science of opioids and how that should influence treatment and policy decisions. Currently he contracts with the Center for Disease Control on the academic detailing of prescribers to educate them on the appropriate use of opioids for the treatment of pain.He continues to work one day per week treating those afflicted by the disease of addiction at Meridian Behavioral Health Services in western North Carolina.  An Interview with Johnathan Goree, MD Director of Chronic Pain and Opioid Stewardship University of Arkansas for Medical Sciences NaRCAD Training Alumnus by Kristina Stefanini, Program Coordinator at NaRCAD Tags: Detailing Visits, Opioid Safety, Training NaRCAD: Thanks for talking with me today! Can you tell me a little bit about yourself and how you ended up in pain management? Johnathan Goree: I’m from Arkansas originally. After completing college at Washington University in St. Louis, medical school and residency at Cornell, and a pain medicine fellowship at Emory, I was recruited to start the chronic pain division at the University of Arkansas for Medical Sciences – 2 miles away from where I went to high school. I’m proud to work in Arkansas; Arkansas is such a poor and rural state, so we don’t often have the resources that other states have.  I went into anesthesiology because I wanted to be the best prepared doctor for an emergency, but I moved into pain medicine because I missed the 1-on-1 patient contact and longitudinal patient care. Here are some other things that lead me into pain medicine. After getting my wisdom teeth removed, I was given too much fentanyl during the procedure resulting in being given Narcan to wake up. That was the first time in my life I experienced 10/10 pain. It allowed me to understand how pain can completely dominate someone’s consciousness. I am also passionate about pain management in minority communities. Many in those communities feel that their pain is undertreated, and evidence backs that up. NaRCAD: As a physician, what are some of the barriers that detailers may have talking to clinicians about pain management? How can these be navigated? Johnathan Goree: Every physician will say the number one barrier is time. While most physicians are excited to learn about anything that will improve patient care, unfortunately, physicians are usually not in control of their schedule.
NaRCAD: How can clinicians act as champions in an academic detailing campaign? Johnathan Goree: One way physicians can help is with the crafting of educational materials. Physicians know how physicians think and can help by crafting a message that may better catch attention. Another is by dedicating time to answer follow-up questions from detailers and other clinicians. In my field of chronic pain management, detailers that don't have a clinical background may not know how to answer questions on specific off-label situations or treatment of specific pains. A follow-up visit or call with a clinician can help with that. NaRCAD: Anything else you’d like to add for our readers? Johnathan Goree: More praise for you guys – your course is excellent! Really understanding the science and method behind academic detailing made me excited to be a part of it. I hope more physicians engage both as detailers and as champions. I think it’s really important. Biography.
Johnathan Goree, MD, Director of Chronic Pain and Opioid Stewardship University of Arkansas for Medical Sciences Board certified in anesthesiology and pain medicine, Dr. Johnathan Goree received his Bachelor of Arts in biology from Washington University in St. Louis. He then moved to New York City where he completed both his medical degree and a residency in anesthesiology at the Weill College of Medicine at Cornell University. Following his time in Manhattan, he completed a fellowship in chronic pain medicine at Emory University Hospital in Atlanta, Georgia. In 2014, Dr. Goree returned home to Little Rock, Arkansas to join the faculty at University of Arkansas for Medical Sciences where he serves as the Director of the Chronic Pain Division and an Assistant Professor in the Department of Anesthesiology. He primarily focuses on the treatment of chronic pain conditions using opiate sparing, minimally invasive techniques. His specific research interests include complex regional pain syndrome, neuromodulation, and the effects of opioid education initiatives on patient outcomes. An Interview with Victoria Adewumi, MA, Community Liason, City of Manchester Health Department NaRCAD Training Alumna by Kayland Arrington, MPH, Program Manager at NaRCAD Tags: Detailing Visits, Opioid Safety, Program Management, Training  Victoria @NaRCAD2018's panel on AD for the opioid crisis. Victoria @NaRCAD2018's panel on AD for the opioid crisis. NaRCAD: How did you get into AD? How was the Manchester team formed? Victoria: I was very interested in community outreach and improving the health and well-being of families! I had cursory experience with substance use disorder management and had to jump in with both feet. It really helped having other detailers on the team that NaRCAD trained that I could lean on. The other detailers constantly provided support, and one helped open the door for me at her health system to speak with clinicians. She even provided me talking points that previously worked for her so I could walk into my first appointment feeling confident.  NaRCAD: What has your experience been as a detailer who does not have clinical experience but who does have public health expertise? Is someone able to be effective as an academic detailer without as much prior clinical training? Victoria: My experience has been extremely positive! I care about community, and I thought this was a great opportunity to gain new expertise in this field. I’ve always felt that a community perspective is needed for us to be able to leverage our impact in this field. The NaRCAD Academic Detailing techniques training was fantastic in helping me build tools to be able to speak well and motivate clinicians around medication-assisted treatment (MAT). My goal as an individual detailer is always to present myself as being on the same team as clinicians. I really see detailing as having a solution for clinicians, rather than simply trying to sell them an idea.  Manchester is located in Hillsborough County, NH Manchester is located in Hillsborough County, NH NaRCAD: Was there a time when a clinician presented pushback or obstacles that made it difficult to get your message across? Victoria: Some clinicians seemed to have already decided whether they were going to be on board or not before I even met with them. I had to feel strong and confident in the skills that I have. When I meet with a clinician, I always frame it as “I’m coming in as a representative of the community. There’s a crisis in our community, and you, as a provider, are a key part of the solution. How can we get you involved?” and “What kinds of things can you tell us that we haven’t even thought about before?” We need everyone’s participation if we’re going to change the tide of the city of Manchester, and clinicians are a vital part of that.
NaRCAD: You have mentioned the power of the team of detailers--can you tell us how the Manchester AD came to be so strong and effective? Victoria: I didn’t know any of the other detailers before the project. The NaRCAD training was great as an introduction to the work and to each other. We all had a sense of hope that was immediately apparent. We have the privilege of doing work that helps save lives and because of this attitude, there was a sense of camaraderie right away. We’ve been effective because our AD team is strong, and it was strong because we were intentional about building bonds. During the implementation period, we never went more than a month without checking in with each other, and sharing successes and challenges. I don’t think I would have enjoyed the process as much if I didn’t have this amazing AD team of colleagues. We’ve had incredible success in building a team of detailers who are all committed to and excited about the work of connecting with frontline clinicians to improve patient care around opioid safety.  NaRCAD: How would you recommend other programs go about recruiting those people that are equally committed and excited? Victoria: That’s a great question! I didn’t necessarily have an opioid response background, but I’ve always cared about communities. That desire to help others makes a great detailer. The trainings can teach the clinical content, but that element of wanting to improve people’s lives is the anchor of a strong AD team, and will resonate with the providers you’ll be detailing. I would then advise new sites to do the important work of helping their detailers to build strong relationships and a sense of teamwork right from the beginning. Those relationships will support everything, from good communication with clinicians, to a renewed sense of purpose in doing the work, which shields against burn out moving forward. Consistent opportunities to check in and connect between AD team members can’t be overemphasized—it truly made me feel that I was never in this alone; I was always working as part of something bigger than myself.  Biography
Victoria Adewumi, MA Community Liaison City of Manchester Health Department Victoria Adewumi is a Community Liaison with the Manchester Public Health Department. Victoria primarily helps coordinate and staff programming of the Manchester Community School Project, a model that facilitates better health for Manchester residents through place-based interventions. Victoria serves Manchester residents by linking them to partners in the health, social service, business, non-profit, and faith communities and by engaging community members in resident leadership and equity activities. Victoria also participates in efforts to serve refugees and newcomers in New Hampshire through both direct service and community-building initiatives. Victoria holds Bachelor and Master of Arts Degrees in Political Science from the University of New Hampshire. Featuring: Mary Nagy, MPH, RN/BSN, Public Health Detailer, HIV Care & Prevention Unit, Michigan Department of Health and Human Services, NaRCAD Training Alumnus Tags: Detailing Visits, Health Disparities, HIV/AIDS, Sexual Health, Stigma NaRCAD: Thanks for joining us, Mary! You’re a Public Health Detailer in the HIV Care & Prevention Unit at the Michigan Department of Health & Human Services. Before we talk about how you got into your current role, can you tell us what you were doing before that? Mary Nagy: I was an ER nurse for five years. During that time I worked all over the country in lots of different settings, but I noticed the same patterns playing out no matter what city I was in. I was seeing patients daily who were either in the last hours of their lives or needing immediate life-saving interventions as a result of medical problems that might have been avoided entirely through basic services or preventative medicine. The longer I worked ER, the more clearly I saw the effect of systemic forces and environment on health, their unequal distribution across society, and the more I wanted to find a way to work towards health equity. I decided to study public health, and earned my master’s degree in Environmental Health Science at the University of Michigan. In addition to giving me the opportunity to design and carry out my own research, the program I did had a strong health policy component, which helped me add to the understanding of healthcare delivery I formed during the time I spent at the bedside. 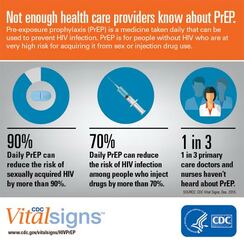 NaRCAD: Tell us what interested you about your current position and what a “day in the life” of a detailer looks like for you. Mary Nagy: I saw the job posted and was immediately interested in it because I think detailing, especially on the topic of pre-exposure prophylaxis (PrEP), is a really effective way to strengthen prevention infrastructure and affect health outcomes. Clinicians are under a lot of pressure and I was drawn to the idea of being a source of relevant, high quality, trusted information. The detailing program here in Michigan is comparatively young and its development is ongoing. Fortunately for me, lots of folks have been willing to help! I've drawn from a broad range of sources has been really helpful during detailing visits, because the needs of providers are so diverse; folks are asking about billing and coding for PrEP visits, standing orders, HIV risk assessment, nuts and bolts of services offered by our state lab, STI screening and trends, and financial supports for PrEP, best practices with PrEP initiation and follow up, and more. I’ve been working hard to broaden my knowledge base, but also to identify resources for questions I don’t know the answers to and topics I’m weaker on.  Image from UNAIDS Image from UNAIDS NaRCAD: Why are you passionate about HIV prevention, and why is academic detailing for HIV prevention so important? Mary Nagy: Even though I’m very new to the field, I think it’s a very exciting time to be doing this work because I do believe it is possible to end the HIV epidemic in the US within the next few decades. Racial and ethnic minorities continue to be underrepresented in PrEP utilization and overrepresented in new HIV diagnoses, and I want my work to contribute to correcting this. I think PrEP can be a tool for health justice and being part of that is valuable to me.  NaRCAD: You’ve mentioned environment a couple of times. Can you tell us how environment is connected to HIV contraction and prevention, if at all? Mary Nagy: I think that’s where my mind goes, because I’ve seen the powerful effect of environment on health, and this is certainly true on a population level. I never want to diminish the power and agency of individuals, but everyone operates under multiple layers of forces. Examples of this include policy, especially the persistent legacy of overtly racist housing policies; the “war on drugs” and resulting mass incarceration; or a justice system that data shows us doesn’t work in the same ways for everyone. These systemic forces, applied to millions of people over many decades, result in the disparities we see in HIV rates, overall health, wealth, and many other areas. Increasing access to PrEP means we can mitigate some risk for folks who might have more exposure due to the environmental context in which they live. For Michigan, one of the ways detailing can help make PrEP easier to access is increasing geographic availability. A large portion of our state is rural, and many counties do not currently have a known PrEP provider. Another challenge is, of course, cost. The cost of PrEP and associated visits and screening tests is a policy issue, and while we hope and expect to see cost come down in the future, in the current landscape, it's important to prioritize educating providers and their staff on available financial supports and how to apply them, so cost doesn’t keep people who can benefit from PrEP from getting and maintaining access.  Image: University of New Mexico Image: University of New Mexico NaRCAD: In addition to geography and coverage, what are some other barriers you’ve encountered when doing academic detailing for HIV prevention? Mary Nagy: Stigma around HIV and other STIs is a big issue. We know that when providers talk openly with patients about their sexual health, they’re better able to accurately assess risk for HIV and STIs and screen and treat appropriately, but those conversations are not happening with enough regularity. Rates of STIs like gonorrhea, chlamydia, and syphilis have been rising, and continue to increase, so there's a lot of opportunity there. NaRCAD: How has detailing been received overall? Are providers open to education on PrEP? When I think about why detailing is important and why I’m doing it, the first thing that comes to mind is a recent survey of primary care providers MDHHS carried out in Southeast Michigan. Providers were asked which supports would best help them to incorporate PrEP into their practice, and "education" was by far the most frequent answer. In addition to the research I’ve seen indicating detailing is an effective intervention to change provider behavior, it's clear that the providers themselves agree that education is important. If we can work with providers to make PrEP available and easy to initiate and maintain, the protection it offers from HIV can improve health outcomes for patients at high risk.  Biography
Mary Nagy, MPH, RN/BSN Public Health Detailer, HIV Care & Prevention Unit Michigan Department of Health and Human Services Mary is the public health detailer for the State of Michigan and conducts direct outreach with medical providers to support HIV prevention strategies and stigma reduction statewide. She received her master’s degree in Environmental Health Science from the University of Michigan School of Public Health where as a Graham Sustainability Fellow her research focused on municipal water quality and affordability. Mary also has several years of experience working in as an Emergency Department RN in trauma centers across the US and her work in health equity is informed by her time as a frontline health worker. Kayland Arrington, MPH, Program Manager at NaRCADTags: HIV/AIDS, Opioid Safety, LOOPR, Training This New Year, NaRCAD has new staff, new partnership sites, and will be addressing critical topics in health. We’ve had a successful 2018, and we’re already working hard to improve patient health through clinician education in 2019.  One of the main topics we provide support on is HIV prevention for high-risk patients. While it is true that rates of HIV are declining in some populations, other groups are still very much at risk for developing HIV. According to the Centers for Disease Control (CDC), half of all black men who have sex with men will contract HIV in their lifetime. These statistics are staggering, and NaRCAD is doing everything we can to help by engaging directly with frontline providers who can communicate best options for prevention directly to their patients. We do this by training academic detailers to meet with clinicians to offer tailored, evidence-based clinician recommendations.  Image Credit: AIDS Coalition of Nova Scotia Image Credit: AIDS Coalition of Nova Scotia In December, we traveled to Las Vegas to facilitate an AD training to increase prescriptions of Pre-exposure prophylaxis (PrEP). PrEP is a daily medication prescribed to people with a high risk of developing HIV. The CDC reports that PrEP reduces the risk of getting HIV from sex by more than 90%; it also reduces the risk of contracting HIV from injection drug use by more than 70%. NaRCAD is continuing our work in 2019 to train health educators to talk to frontline clinicians about the benefits of prescribing PrEP to their high-risk patients. Our first training of 2019 is in February at the PrEP Public Health Detailing Institute in San Francisco, hosted by our partners at the San Francisco Department of Public Health.  We’ve also added on 2 new sites to our county-level LOOPR Partnership! We will be traveling to St. Francois County, Missouri and Ware County, Georgia in March. The CDC has identified 220 counties (5% of counties in the nation) that are at highest risk of HIV and/or Hepatitis C as a result of the opioid crisis. St. Francois County, MO is ranked 69 out of those 220 counties. Ware County, GA is located in the southeast corner of the state and doesn’t have as much access to resources as counties more centrally located. NaRCAD is excited to join both of these high-burden counties in their efforts to reduce harm from the opioid crisis.  One element that is a common thread with both HIV and the opioid crisis is the fact that these are both highly stigmatized clinical topics. Along with community stigma, clinicians themselves may be inadvertently biased against patients with substance use disorder and/or those at high risk for developing HIV. As the result of a fear of stigma, it’s also common for patients to refrain from sharing high risk behavior with their providers. To ensure that front line clinicians increase PrEP prescribing and work to treat pain in safer ways, the academic detailers we train this year will also explore ways to address clinician stigma. Along with our county-level support, we’ll also travel to Tennessee, Oregon, and Maryland this year. And as always, we’ll hold our usual Boston home trainings in May, July, and September before our year comes full circle at our 7th Annual International Conference on Academic Detailing in November. No matter how we connect in the year ahead, our entire team is looking forward to supporting you in 2019—let us know how we can help, and stay tuned for more updates here on the DETAILS Blog.  Biography
Kayland Arrington, MPH | Program Manager, NaRCAD Kayland earned her Master’s Degree in Public Health from Boston University, with concentrations in Health Policy and Law and Maternal and Child Health. She has experience coordinating suicide prevention and awareness programs. She also has experience in health promotion and education on topics ranging from substance use disorder to sexual violence. Kayland is passionate about improving access to resources, supporting population health programming, and is an advocate for evidence-based medicine. Read More. A ROADMAP for Detailing Success: Improved Outcomes for the Medicaid Population in Oklahoma12/7/2018 Guest Blogger: Jacki Travers, PharmD Clinical Academic Detailing Pharmacist Pharmacy Management Consultants NaRCAD Training Alumnus Tags: Detailing Visits, Mental Health, Pediatrics In June of 2015, I had never even heard the term “academic detailing.” If you’d asked me to define it, I might have said it had something to do with the relationship between teachers and their cars. Little did I know that I was about to become an academic detailer, embarking on an exciting, rewarding, and sweaty-palmed journey to bring evidence-based materials to providers across the state of Oklahoma.
The Oklahoma Medicaid population is mostly under age 21. Detailing topics have included treatment of ADHD, use of atypical antipsychotic medications, and decreasing the use of antibiotics for treatment of upper respiratory infections. We are a small program by comparison, having one full-time detailer since 2015. We added one quarter-time detailer within the last year.  I will share some specific activities that worked for us, which creates a ROADMAP that has served us well and may help you as you begin or enhance your detailing efforts. R – Review When each set of materials neared completion, we asked the experienced NaRCAD staff to review our materials. Having an outside source helped clarify any confusion and identify ways to help the AD visit flow more naturally. O – Objectivity In identifying providers, we were making a bit of a judgement about their prescribing. As a detailer, I found it unhelpful to bring these judgements into the detailing visit. It is important for providers to see detailers as an ally for change rather than a source of punishment or criticism. A – Acceptance We surveyed providers’ acceptance of the program with each AD visit by asking them to evaluate the detailer and the materials. We also asked if they were willing to participate in future visits and recommend the program to colleagues. D – Define Defining the expected care gaps helped guide creation of our key messages. The treatment guidelines for ADHD are well established and remain unchanged since 2011. Comparing these guidelines to national and state patterns gave us a starting point for developing key messages. In addition to published guidelines, evaluation measures such as the Healthcare Data and Information Set (HEDIS) were very helpful. Doing this examination on the front end helped us begin with the end in mind and ensured we collected data we needed from the start. M – Motivational Interviewing Motivational interviewing (MI) is a communication style that is used to modify behavior. MI techniques helped us avoid some of the pitfalls that can accompany potentially confrontational conversations. A – Appealing Graphics We use Adobe Creative Cloud, which we find it to be very user-friendly. For someone with no graphic design experience, YouTube training videos were very helpful. We also use Pixabay as a source for ready-made graphics. All materials are open source and royalty free. We looked at the graphics used by other programs and even materials distributed by pharmaceutical representatives. Having appealing graphics is necessary for any AD program. P – People Having professional mentoring has helped move our program to the next level. Specifically, our detailers received invaluable preparation from the excellent NaRCAD Training Series. Moreover, I never miss the chance to learn from all the presenters and breakout participants at the International Conference each year. We are encouraged by the outcomes we have seen to date. The ADHD campaign produced a 58.33% reduction in medication claims for the very young (age 0-4) and cost savings of more than $226,000 across all ages. The antipsychotic campaign produced a 19.51% reduction in medication claims across all ages with associated savings of more than $365,000. I hope this snapshot of our program demonstrates that even small AD programs can show sizeable improvements in health outcomes and improve utilization of healthcare resources. Now, more than three years later, my understanding of academic detailing is much deeper and continues to grow with each new challenge. I was not completely wrong in my definition though: I absolutely see myself as a teacher and I certainly spend a lot of time in the car!
Exercising Empathy, Planting Seeds: An Interview with the Manchester, NH Academic Detailing Team10/26/2018 Featuring: Carol Furlong, LCMHC, MAC, MBA, Director of Substance Use Disorders, Elliot Hospital Jill MacGregor, APRN, Catholic Medical Center, & Katie Sawyer, LICSW, MLADC, Director, Integrated Treatment of Co-Occurring Disorders, Network4Health/Mental Health Center of Greater Manchester Interview by Isabel Evans, Fellow, NACCHO, in partnership with NaRCAD  Tags: LOOPR, Opioid Safety, Stigma, Substance Use, Training EDITOR'S NOTE: Manchester, New Hampshire, was the third site of four selected for a 2018 pilot program of the CDC (Centers for Disease Control and Prevention), NACCHO (the National Association of County and City Health Officials), and NaRCAD (The National Resource Center for Academic Detailing). This exciting pilot program focused on community-level work with local public health departments to develop customized interventions to reduce opioid overdose and death. Four sites experiencing significant public health problems related to opioids were selected to be trained in academic detailing; those trained health professionals then conducted 1:1 field visits with front line clinicians to impact behavior around prescribing, treatment referrals, and patient care, with Manchester’s team focusing primarily on access to Medication Assisted Treatment [MAT]. As year 1 comes to a close, we’re showcasing successes from the field. Thanks for talking with us about your work in Manchester, New Hampshire. Can you tell us about your team? How were detailers chosen to represent the health department for this pilot project? Carol: Tim Soucy, from the Manchester Department of Health, contacted representatives at each of our organizations and gave a little bit of information about the training. He asked if our organizations had particular people that might be interested, and my supervisor thought of me, since I was in the middle of developing a MAT program for my organization. I jumped at the chance to participate. Jill: My organization received the same email, and as the primary care lead nurse practitioner, I was considered the most appropriate to participate. Katie: The invitation came from the site that received the CDC grant (City Health Department). The invitation was disseminated among a number of local human service/health agencies who are part of a Network of agencies as a result of our 1115 Waiver partnership.  The NaRCAD team came to your site back in March, 2018, helping you get ready to be ‘in the field’ and talk to clinicians about the opioid crisis. Tell us how that went, and how you applied what you learned in training. Carol: I’m a naturally shy person who dislikes being the center of attention, so I was incredibly nervous about the role plays during training. The turned out to be invaluable, since I use the skills I developed through practicing and receiving feedback during every visit. The role plays prepared me so well for meeting with providers, and I go into the conversations feeling confident and comfortable. When they ask questions, I feel that I know how to answer, or where to turn for more information, such as the wonderful handouts available on the NaRCAD website. Jill: For me, learning how to hold a discussion as a detailer was the most important element of the training. I learned how to frame a conversation using open-ended questions, which allows the discussion to progress. Understanding how to simultaneously get a provider’s perspective, while also giving them the information they need, is a critical detailing skill. Katie: We were able to role play, which has proven very helpful out in the field to stay focused, on topic, and empathetic to the position of each clinician that I speak to. The handouts that NaRCAD provided have easy to read information and great graphics, so they have also proved useful for staying on track with the key messages during detailing visits, along with providing supplemental information. 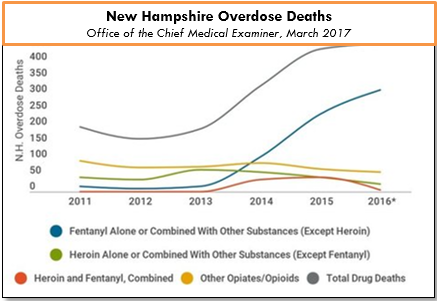 The opioid epidemic has affected many communities in unique ways. How have local clinicians responded to your visits? What do clinicians in Manchester see as major barriers to improving health for their patients struggling with this issue? Carol: Clinicians can be a little skeptical at first, since they’re often expecting that I’m going to try to “sell them” on something. When I focus on listening to their experiences and their concerns, I’m able to gently address those concerns and give resources or suggestions. Even just having a discussion can help clinicians to feel that you’re interested in how they feel, and that you genuinely want to help them – I would describe some clinicians as “dumbstruck” from our conversations, because they’re preparing to do battle with me, but they instead come to see me as a resource, and are more willing to meeting with me. As for challenges, we deal with a fair amount of stigmatization of substance use. It’s a major barrier, and we’ve had to spend a lot of time addressing that in my organization. Another barrier for clinicians is a preconceived notion that providing MAT is an onerous process, and too time-consuming to add into their schedules. And these two barriers really complement each other in a bad way – I often get providers saying that MAT is too much work and that their MAT patients will just end up using opioids again and ending up back in the emergency room. Breaking down these misconceptions about MAT and getting to the root of the stigma against MAT is a big challenge. However, we’re approaching these challenges with education and lots of conversations, since we’ve found that helping our staff to get a better sense of addiction as a disease is really invaluable to making them more open to MAT and treating people with opioid use disorder. The timing of the academic detailing initiative couldn’t have been better for my organization, because having conversations about addiction leads well into having conversations about MAT, and vice versa. Engaging in academic detailing has opened up a whole new avenue of clinician education for me. Jill: Because of my role at my health system, I talk to providers about many different topics and they’re used to me approaching them, which has definitely helped give me and automatic “in” and bring up sensitive topics. My institutional knowledge helps too, since I can answer questions specific to my organization and our various programs or resources around opioids.  A major challenge I face is that providers don’t think they have the time and resources to implement MAT into primary care, and they don’t feel they have the behavioral health support to do so successfully. However, I’ve found that this is often based around a lack of knowledge, since when I ask more probing questions about MAT, it’s often clear that they don’t really know much about it! Providers will come to conclusions without getting the right education, and I find that they often “change their tune” when I give them more information. Providers are also hesitant about writing a prescription for a MAT patient if there isn’t someone in their office who can talk to the patient about addiction itself. Right now, we’re working on integrating behavioral health clinicians into primary care, which I’m hopeful will help with this very real concern. Katie: There has been some hesitation in sharing with detailers, in regards to professional experience, as I believe most clinicians are on edge in trying to do the best that they can to address patient needs, while also supporting alternatives to typical or historical use of prescribed opioids. With an empathetic and interested stance, I’ve found that most clinicians are open with their experience and struggles. There are a number of themes among clinicians for challenges that I’ve noticed, including a limited behavioral health workforce to support what they view as an ideal MAT protocol, which would include individual and group counseling, regular urine toxicology screens, and wraparound services along the continuum of care. In addition, there is a concern among providers about the potential diversion of Buprenorphine by patients.
Katie: It has been rewarding to meet with each clinician for different reasons – I would view success as learning more about the clinicians that are already on board and excited to pursue getting a waiver, as it gets them talking and feeling a renewed energy to share with others. I view my conversations with clinicians who are not interested in pursuing a waiver as equally rewarding, since it allows for both of us to share and hear the other’s perspective. We can agree that the work is needed and challenging, no matter how we decide to go about addressing the needs of our patients. Lastly, what advice would you tell new detailers? What do you wish you knew when you started out? Carol: I would tell new detailers to take a deep breath and know that you’re ready for this – NaRCAD does such a good job of training us as detailers, and you just feel ready. Jill: I would say to recognize that everyone has a natural process for adapting to new ideas. You’ll get some providers who are ready and energized, some who will want to watch others in action before they jump in, and some who simply may not be interested. It can be frustrating when providers aren’t interested in your topic or resources, but understand that this is natural, and don’t take it personally! Every visit will be different, and that’s okay. Katie: My advice is to remember that success is not defined as “convincing” someone that the topic of your detailing visit is “the right answer”. In fact, trying to convince another person of anything is essentially walking against waves. Instead, be open to listening to that person and their experiences, and then value the experience that they have had. This is more likely to open the conversation to allow you to share your wealth of information and experiences. It’s all about planting seeds. Ideas? Comments? Questions? Sound off on this blog in the comments section below!
Opening Up the Conversation: An Interview with the Bell County, Kentucky Academic Detailing Program10/26/2018  Featuring: Robin Tuttle, RN, ER Nurse, Academic Detailer, NaRCAD Training Alumnus Interview by Kabaye Diriba, Senior Program Analyst, NACCHO, in partnership with NaRCAD Tags: Detailing Visits, LOOPR, Opioid Safety, Rural AD Programs EDITOR'S NOTE: Bell County, Kentucky, was the first site of four selected for a 2018 pilot program of the CDC (Centers for Disease Control and Prevention), NACCHO (the National Association of City and County Health Officials), and NaRCAD (The National Resource Center for Academic Detailing). This exciting pilot program focused on community-level work with local public health departments to develop customized interventions to reduce opioid overdose and death. Four sites experiencing significant public health problems related to opioids were selected to be trained in academic detailing; those trained health professionals then conducted 1:1 field visits with front line clinicians to impact behavior around prescribing, treatment referrals, and patient care, all within a rural area. As year 1 comes to a close, we’re showcasing successes from the field. Thanks for talking with us about your on this pilot project with NACCHO, the CDC, and NaRCAD, working to support local efforts in your community. Robin: What we’ve been doing has been a breath of fresh air! I'm proud to be a part of it, and happy to help in any way that I can. Tell us how local detailers were selected for this project—what kinds of professional backgrounds make up your diverse team members? Robin: I was asked by a co-worker, another detailer, who thought “I know this really outgoing, outspoken person that might fit the team.” Our team is made up of people that have hands-on knowledge about the opioid epidemic. I’ve been in healthcare since 1988 and I’ve been living here in Bell County for 30 years. I started working as a nurse aid at one of the local hospitals and then went on to college to get my RN. Our detailing team all had a common interest when we got together.  What elements of the training do you apply most often during your visits when delivering your key messages? Robin: What helped me the most was that last day of training when we were practicing academic detailing. Asking open-ended questions is the most important thing. You get so wrapped up in wanting to deliver your messages, but it’s not necessary that you get all of your messages in on that first visit. You may feel rushed to deliver all your messages if you’re afraid you’re not going to make it back in the door, but what I found is the more I met with doctors, and the more I said things like, “What have you seen in your practice?” or “Tell me about a patient…” or “Talk to me about the problems you’re having…”, the more I saw the conversation open up. That’s something I really picked up on the second day of training—learning to turn it back around and asking [needs assessment] questions. Let them get involved, and let me really listen to what they have to say; that way it'll help contribute to the conversation going forward. The opioid epidemic can be a sensitive topic. When you approach clinicians to discuss their behaviors around the opioid epidemic, how are you generally received? What do clinicians in Bell County see as major challenges in your community? Robin: Almost everyone I spoke to was very receptive about everything that we talked about, including all 5 of our campaign’s key messages. Because treatment in this area is slim to none, it all circled back to, “What if I find someone [a patient] that has opioid use disorder? How can you help me?” Doctors here are telling me that even people that have overdosed and come to the hospital are having a hard time [getting access to treatment]. There are places that are not in Bell County, but we would need some sort of transportation system that could get patients to those places.  What challenges do Bell County clinicians face, along with being busy, when trying to support their patients who are prescribed opioids? Robin: Clinicians are often challenged in identifying symptoms of someone with opioid use disorder. Also, sometimes patients are sent to a pain [management] clinic, but those don’t always work. In our community, we can send them to the local Suboxone clinic which is accessible and easy to get to. When it comes to Suboxone, you cannot look at it as an “all-or-nothing” approach. That’s a challenge here in Bell County, trying to get the community to know that abstinence is not always the answer, and sometimes people might have to take some form of medication for life to get the wiring back together that they've already lost because of their disorder. I also understand some of the doctors are adamant about their current patients that have been taking these medications for 25 years for this chronic pain, which they don’t think they can do much about, and they’re concerned about this newer generation [of patients] coming in. What have been some of the more rewarding exchanges you’ve had with clinicians you’ve met with? Robin: I've had a lot of good visits, but this one sticks out in my mind: there was one clinician where I felt immediately like I was going to get the “brush off”. But I ended up staying for an hour and a half! I sat there with this doctor, who I’ve had a challenging professional relationship with historically, and he ended up talking to me at length about patients he was seeing, and those he had inherited. I was so excited that I’d spoken with him for so long, and that I’d covered all 5 of our campaign’s key messages. I walked away from that visit with questions to follow up on that I wanted to be able to answer for him at a future visit, and I felt like I made a new friend. What do you want to tell new detailers who are just starting to form teams and try this kind of 1:1 outreach education model out with clinicians in their communities? What piece of advice would you have appreciated when you started your first detailing visits? Robin: Try not to get discouraged! After we divided up all the physicians, we started making phone calls. That can be discouraging. I found out we actually had more luck stopping by. We called it the “drug representative look”: you dress up, put your badge on that says academic detailer, have the clipboard and all the paperwork, and you look professional. I really found out that I had more luck by just walking in and saying, “Do you have a minute?” Don’t get discouraged if you're making calls all day long and they keep putting you off, because receptionists are making appointments all day long too and it’s hard to explain what you’re doing over the telephone. We definitely felt discouraged during the first couple of weeks of outreach. We were feeling like we hit a brick wall, and that’s when we coined the term "drive-by” detailing visits. We started driving around and just showing up at offices. So, get out and drive if you can’t get through over the phone. Go with a card and introduce yourself. They [clinicians] all want to talk about opioids. You'll be surprised when you get in the room with them and they start talking. Ideas? Comments? Questions? Sound off on this blog in the comments section below!
 Tags: Detailing Visits, Evidence-Based Medicine, Materials Development, Jerry Avorn Here’s the good news: academic detailing is becoming so widely accepted that everyone wants to help provide the evidence that is disseminated. That’s also the bad news; worrisome examples range from the grotesque to the sinister. One eminent health policy expert wanted to know how much it would cost to put together a nationwide academic detailing program (my heart leaped) that would be underwritten by the pharmaceutical industry (dammit). Prescription drug management (PBM) companies now offer so-called academic detailing services as part of their contracts with payors to oversee drug choices and spending. Sounds good until one realizes that a large chunk of PBM revenue come from payments by manufacturers to move market share to their products. So much for communicating evidence that is neutral, unbiased, and non-commercial. You’d think we’d have learned our lesson by now. Do universities or insurers or government fail to offer enough continuing education about prescribing? No problem, drugmakers will be more than happy to fill the gap, either for free or at amazingly low cost…. often with really great food. That local clinical expert who shows up at Grand Rounds to provide an overview of all the new treatments for diabetes, at no cost to the hospital? Don’t ask who’s paying him to be there. And those convenient smartphone apps that provide so much handy dosing information for any drug you can think of? All you have to do is read the commercial messages that pop up on your way to the data, as the vendor promises its pharmaceutical sponsors the chance to "embed your brand message at multiple points across the care continuum."  There is a solution to the concern about who’s providing the content for academic detailing programs, and it’s much easier than figuring out whether a particular Facebook ad is brought to you by a Russian bot. Just expect that any purveyor of AD information will reveal clearly all the financial ties it and its authors have with any drug or device maker, in relation to program sponsorship as well as the creation and editing of the clinical content. After years of being misled about hidden data on adverse events or failed studies, we’ve developed a higher set of expectations about disclosing all information about clinical trials, and the need to reveal authors’ financial ties for published studies. Those same higher standards must also be applied to academic detailing programs, so that its audiences will know whether the material is the carefully vetted work of a team of unconflicted reviewers who don’t work for any manufacturers, or is instead yet another terribly sophisticated new way to market particular products. Want more? Peruse the archive of Jerry's pieces here on DETAILS. _____________________________________________________________ Biography.
Jerry Avorn, MD | NaRCAD Co-Director Dr. Avorn is Professor of Medicine at Harvard Medical School and Chief of the Division of Pharmacoepidemiology and Pharmacoeconomics (DoPE) at Brigham & Women's Hospital. A general internist, geriatrician, and drug epidemiologist, he pioneered the concept of academic detailing and is recognized internationally as a leading expert on this topic and on optimal medication use, particularly in the elderly. Read more.  Guest Blogger: Joseph Leishman Academic Detailer/Masters in Public Health Candidate Center for Clinical Management Research, Ann Arbor VA The University of Michigan School of Public Health NaRCAD Training Alumnus Tags: Cancer, Detailing Visits, Materials Development, Training  NaRCAD: How did you get into AD? What were you doing before? Joe: I’m a graduate student at The University of Michigan School of Public Health studying epidemiology. As a student I started working at the Ann Arbor VA Center for Clinical Management Research on a lung cancer-screening project. Our project involves 8 different VA sites across the country. As we shifted into an implementation phase, academic detailing was selected as an implementation method. I transitioned to an academic detailer role because of my background in epidemiology, my understanding of lung cancer screening (LCS), and my ability to communicate these principles. I attended the NaRCAD academic detailing techniques training and things took off from there!  NaRCAD: Why is AD for lung cancer screening so important? Joe: Lung cancer screening can be more complex and complicated compared to other preventative services, and most primary care physicians have very limited time to discuss lung cancer screening with patients. There are a number of potential downsides to screening – false positives, overdiagnosis, invasive procedures, and complications from invasive procedures. The benefits of the screening outweigh the challenges, and we have developed a tool for doctors to quickly evaluate a patient’s lung cancer risk, facilitate shared decision making, and make personalized screening recommendations. NaRCAD: Tell us about the lung cancer screening detailing aid and related tools that you made with NaRCAD’s support. How was the process of developing the detailing aid? Joe: Our detailing aid contains background information on lung cancer screening and some of the key evidence behind our tool. It also outlines some of the reasons and benefits behind using this risk-based approach. We tried to keep the detailing aid simple enough that doctors could quickly understand the concepts with little or no additional explanation. This was our group’s first attempt at making something like this. We worked with NaRCAD during the creation of the detailing aid to improve the clinical content, layout, and language. There was a lot of trial and error to create the detailing aid. We ended up going through 10 versions before it was finalized.  NaRCAD: How did you decide what information was most important to put on your detailing aid? Joe: Initially, we started out with too much information. It was too complicated and wordy to effectively communicate our message. We tested it out with our team to see if our message was clear. It was obvious when sections of detailing aid didn’t work well. We really had to focus on narrowing down the main evidence and messages we wished to convey. We used the primary lung cancer screening evidence from the US Preventative Task Force and the National Lung Screening Trial. Our tool goes a step beyond screening eligibility to look at individual risk, life expectancy, and patient preferences, which help providers get past some of the difficulties and complexities of lung cancer screening.  NaRCAD: How does your website complement the detailing aid when you are 1:1 detailing? Joe: A link to the tool is embedded in the Computerized Patient Record System (CPRS), the EMR system that the VA uses. However, it can be also accessed outside the VA with a URL. What I typically do is I have PCPs pull up the website in their workspace after going through the detailing aid. I have providers role play with a sample patient, and I demonstrate how the tool could be used for that specific patient. Using the actual web tool in a detailing meeting really helps to reinforce our message. We feel like it increases the likelihood that it’ll be adopted in an actual clinical practice. NaRCAD: How have clinicians been responding to your campaign? Joe: So far there has been a decent response from the doctors we have worked with. Some of the doctors in the VA have met with detailers before which makes the initial contact easy. However, the most majority of the doctors I have met were receptive to my visits. We’ve been tracking the use of our tool before and after academic detailing at a site level. We don’t have exact numbers, but there has been an increase between before and after AD. We’d be happy to share more complete data in a future blog post. NaRCAD: That'd be terrific, we'd love to share that when it's ready! What other reflections do you have from this process that you'd like to share with our community?
Joe: Academic detailing is a new approach for our group. It has been a real learning experience for discovering what does and doesn’t work and how to best address provider needs. For me, going through this process has been a lot of fun. I love talking with doctors about their struggles and being able to offer a tool that can help them better handle lung cancer screening with their patients. 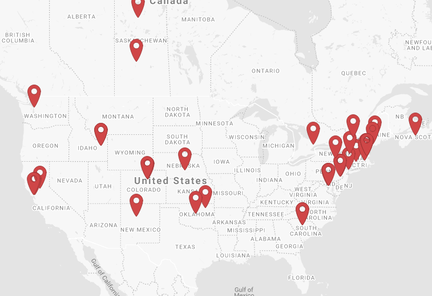 Click the map to check out our partner programs. Click the map to check out our partner programs. Annual Conference, Off to Vegas for an HIV PrEP Training, & Our Team is Growing (and Hiring!) Tags: Conference, Training A letter from the staff at NaRCAD At NaRCAD, we're getting ready for our busy season, which lately, has become a season that lasts all year long. And we're happy for it--because that means we get to help more programs across the US and Canada figure out the most impactful ways to use academic detailing to promote sustainable change. Whether public health programs are looking to increase prescriptions of HIV PrEP for patients at high-risk, encourage more referrals to nutritionists for patients with diabetes, or improve access to treatment for people struggling with opioid use disorder, we're there to help them, from program conception to implementation and evaluation.  Improving HIV Prevention, one training at a time. Improving HIV Prevention, one training at a time. You may know that we offer bi-annual trainings here in Boston for health professionals to learn the techniques of academic detailing with our team of clinical outreach education experts through our 2-day, intensive, hands-on course. But did you know we also travel across the country to train teams on-site in their own communities? Through a partnership with the CDC, NACCHO, and previous funding from AHRQ, we've been on the road for countless successful trainings in early 2018, and we'll be wrapping up the year and heading into 2019 with a bang! Our next stop is Las Vegas, to work with the Southern Nevada Health District on improving outcomes around HIV prevention this December. (And for once, we hope that "what happens in Vegas" doesn't "stay in Vegas"; our goal is to increase visibility and prescribing of HIV PrEP so that more clinicians everywhere are reaching the patients who need it most.)  Click to see our latest agenda! Click to see our latest agenda! Prior to December, we'll be busy here on our home turf for the fall, holding our now-full Fall Training on October 1 + 2, and our fantastic, annual international conference on AD on November 12 & 13. We hope you'll keep your eyes out for dates for our Spring 2019 Training (which will be announced by November!) and that you'll join us for our conference--this year is our 6th annual, and we're excited to announce our full agenda is live on our Conference Series page. Register today--space is limited for this event!  And visit our blog often--we'll be featuring new interviews this fall, showcasing best practices on topics like reducing polypharmacy, reducing opioid prescribing in rural counties, and increasing lung cancer screenings. Want to be featured? Contact us and tell us what you're working on! Our team is ready to custom-tailor our support, so we can offer you the best ideas, resources, and tools to help your program thrive.  We can't wait to see you this fall!
-The NaRCAD Home Team (PS: Want to join our team as a Program Manager? Send us your resume & cover letter.) Director’s Letter: Mike Fischer, MD, MS 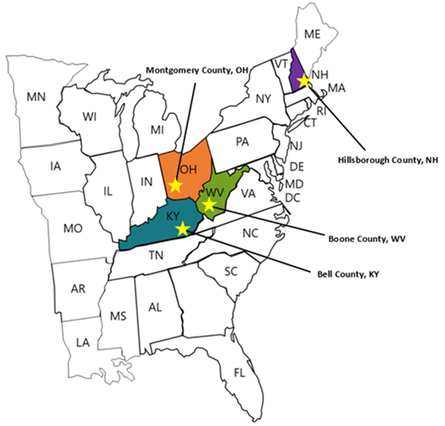 Tags: Director's Letter, LOOPR, Opioid Safety, Rural AD Programs, Training The opioid crisis has been recognized as a major national public health problem, but it actually reflects a collection of many thousands of local crises playing out in individual cities and counties. Each region faces a distinctive set of challenges, driven by economic and social factors, local medical practice patterns, political environment and pressures, and many other considerations. Identifying and implementing effective solutions to address the opioid crisis requires developing an understanding of how these individual challenges interact, and what strategies are most effective in specific situations--one of which is academic detailing.  The NaRCAD team is partnering with the CDC (Centers for Disease Control and Prevention) and NACCHO (the National Association of City and County Health Officials) on an exciting pilot program working with local health officials to develop customized interventions to reduce opioid overdose and death. Four sites experiencing significant public health problems related to opioids were selected: Boone County, Kentucky; Bell County, West Virginia; Manchester, New Hampshire; and Dayton, Ohio.  Public health officials at each site identified a wide range of local stakeholders to participate in developing a community action plan and recruited trainees to complete NaRCAD’s academic detailing training course, which we customized to address the unique challenges that each community faces. We also developed a specialized online toolkit for these sites, including discussion boards, local resources, and printable resources.  A trainee from Bell County, Kentucky, delivers a key message. A trainee from Bell County, Kentucky, delivers a key message. We traveled to each site in March and April of this year, facilitating hands-on trainings in the techniques of academic detailing in alignment with the CDC prescribing guidelines. Trainees came from diverse backgrounds, including pharmacists, nurses, public health officials, and students in the health professions, including pharmacy students, dental students, and medical school students. Plans for implementing AD varied by site depending on the local health care environment; some sites focused more heavily on appropriate prescribing of opioids by clinicians, while others prioritized increasing referral rates for patients with opioid use disorder (OUD), including access to medication-assisted treatment (MAT).  Practicing a concise introduction in Manchester, New Hampshire. Practicing a concise introduction in Manchester, New Hampshire. As the AD trainees at each pilot site continue their work in the field, we’ll learn more about how these diverse strategies succeed, and how we can support adaptations to make academic detailing more impactful. This important collaboration has allowed us to form invaluable partnerships with CDC and NACCHO, leveraging national resources to improve local responses to this epidemic through plans that respond more precisely to local needs and priorities. We’re excited for this pilot program to serve as a model for future opioid safety AD interventions, and we’ll be providing updates here on the blog. In the meantime, tell us: what's happening in your local community around the opioid crisis? Sound off in the comments section below, and let us know if you think clinician-facing education could be a strategy that would improve outcomes for your community. And join us for our next training and our terrific annual conference to learn more about this and other exciting AD projects. -Mike  Biography.
Michael Fischer, MD, MS | Director of NaRCAD Dr. Fischer is a general internist, pharmacoepidemiologist, and health services researcher. He is an Associate Professor of Medicine at Harvard and a clinically active primary care physician and educator at Brigham & Women’s Hospital. With extensive experience in designing and evaluating interventions to improve medication use, he has published numerous studies demonstrating potential gains from improved prescribing. Read more.  Guest Blogger: Monica Mais, MSN, FNP Family Nurse Practioner/Academic Detailer California Opioid Safety Network, Fairchild Medical Clinic NaRCAD Training Alumnus Tags: Detailing Visits, Opioid Safety, Rural AD Programs, Training In 2011, I went from 15 years as an Emergency Room nurse to a new role as a Family Nurse Practitioner in a rural healthcare setting. I couldn’t believe the amounts of prescribed opioids that were coming out of our little clinic—the average chronic pain patient was receiving 240 Morphine Equivalents/day (MEDs), and many of these patients had been receiving these medications for years without oversight. In 2013 I introduced an evidence-based protocol and policy for safe prescribing of Opiates for Chronic Non-Cancer Pain (CNCP).
However, patients who could not obtain opiates from our clinic quickly moved on to the clinic across town. This influx of opiate seeking patients was reason for concern from those receiving clinics. My colleagues and I opened our doors to neighboring clinics and providers and began sharing our policies and successes. Many other area clinics started adapting our policies to their own practice, reducing their opiate prescribing as well.  We formed a coalition called Siskiyou Against Rx Abuse (SARA), and based on our previous successes, we were all shocked to see data showing our county was among the highest opioid prescriptions per capita in California, and had a high overdose rate per capita, despite our efforts. Clearly, more needed to be done! Our coalition facilitator, Maggie Shepard, RN, along with our medical director, Dr. Sam Rabinowitz, and myself were all invited to attend training to become Academic Detailers in San Francisco with the San Francisco Department of Public Health, a partner with NaRCAD, the National Resource Center for Academic Detailing. We did scripting and role-playing throughout the training, learning the important social marketing and communication skills needed to conduct a personalized visit with a provider where the goal would be to change behaviors to continue to promote safe opioid prescribing, Naloxone, and Buprenorphine out to providers in our area. During the training, I was videotaped during a practice role-play, which was very helpful, as it reminded me to speak more slowly, and to organize my key messages and talking points. After the training, getting our detailing program into the field involved a step-by-step process. Here are important things to consider that have worked well for my detailing process:
I plan to continue AD throughout 2018. I believe we have experiences that we can share to encourage our colleagues to make positive changes in in their prescribing habits. Academic Detailing works due to mutual respect of one another’s experiences, professionalism, and willingness to receive new information—it’s an excellent way to foster change within a system! Biography
Monica Mais, MSN, FNP Family Nurse Practioner/Academic Detailer, Fairchild Medical Clinic Monica Mais is a Board Certified Family Nurse Practitioner working at an FQHC in Siskiyou County, located in far Northern California on the Oregon border. She is a founding member of Siskiyou Against Rx Abuse, member of the California Opioid Safety Network and an X-Waived prescriber, working with chronic pain and opioid dependent patients. As a former Emergency Room Nurse for 15 years, many of Monica’s shifts involved witnessing overdoses, drug-seeking behavior, violence, desperation, and healthcare worker burnout. It had been escalating every year to its current crisis level, and Monica wanted to be part of the solution to this heartbreaking epidemic. Questions on this piece for Monica Mais? Contact her at mmais@fairchildmed.org, or leave your thoughts in the discussion forum below. NaRCAD & Training Facilitator Loren Regier, BSP, BA  Tags: Detailing Visits, International Our team's training facilitator Loren Regier recently shared these pearls of wisdom about talking (and listening more) to front-line clinicians. In 1:1 academic detailing visits, detailers have the challenge of finding the right balance between sharing information and acquiring insight into a clinician's practice. It's the kind of balance an expert detailer can execute well, but how? Loren's tips on talking more when necessary to draw out the clinician's needs by asking good questions, and toggling to actively listening and talking less to understand clinicians' biases, are below. Talk More: -If someone is at the point of having “bought in” to a concept/idea, they may just need information. In this situation, it's okay to talk a little more, especially if you sense the “thirst for relevant information.” Talk Less: -If, however, a person has not yet bought in to an idea, it is often more important to talk less, or move towards equalizing the talking. -They will reject too much information that they don’t believe. But in discussing, there is the chance to explore ambivalence, raise doubts, and compare notes. -In all cases, learn to listen and listen well. -I What quick tips would you share with other detailers on assessing needs? Sound off in the comments section below! Biography. Loren Regier, BA, BSP
Clinical Director, Academic Detailing Service, Centre for Effective Practice, Program Coordinator, RxFiles Academic Detailing, U of S, College of Pharmacy/Nutrition, Facilitator, Educational Outreach/Academic Detailing Training | Loren is the Program Coordinator of the RxFiles Academic Detailing Service in Saskatoon, SK, Canada. Loren has guided the development of this provincial academic detailing service since the first pilot project began in 1997. Loren is active as a member of the Canadian Academic Detailing Collaboration and provides training and consultation to various programs and initiatives. Read more. |


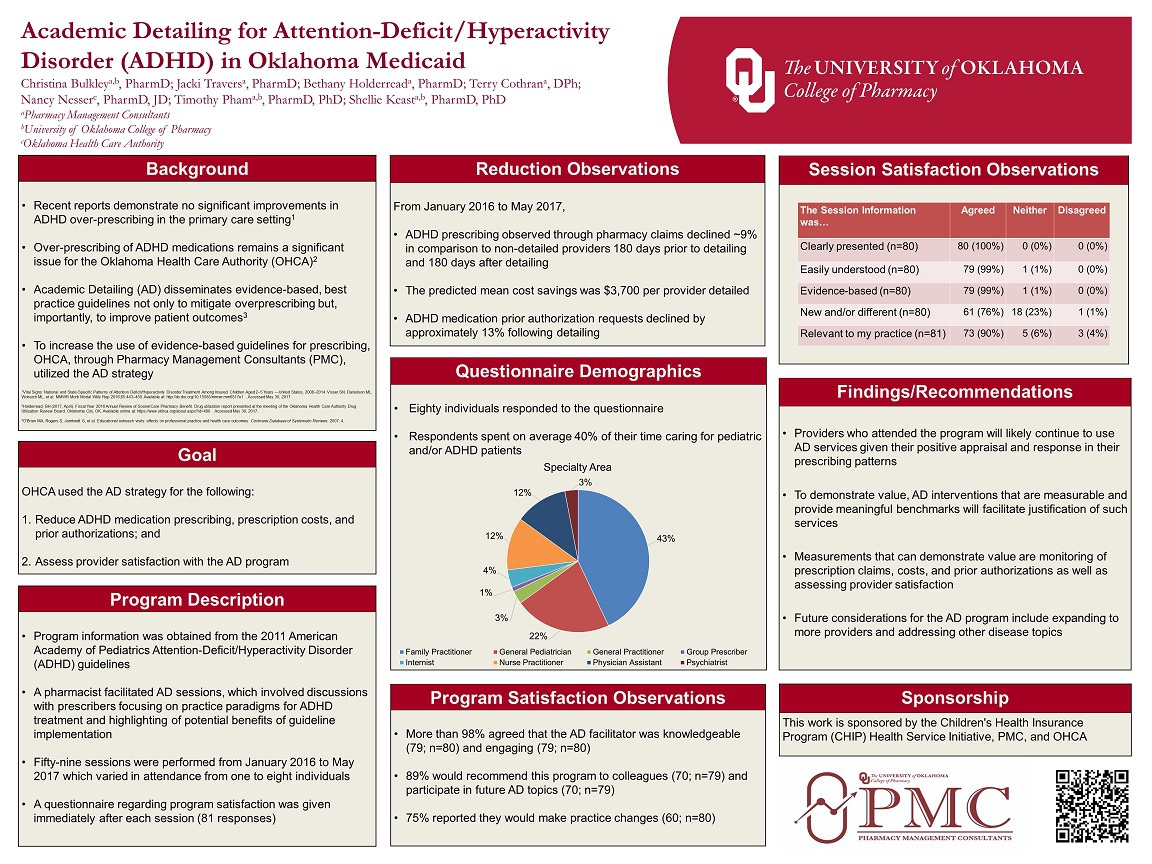{kind=link}