The DETAILS BLOG
Capturing Stories from the Field: Reflections, Challenges, & Best Practices

|
Jerry Avorn, MD | NaRCAD Co-director Tags: Detailing Visits, Evidence-Based Medicine, Jerry Avorn, Primary Care There was a brief shining moment starting in the early 1970s, when I was finishing medical school, that lasted into about the mid-1980s. Primary care physicians (PCPs) seemed poised to rise above their lowest-in-medicine stature to become recognized for playing a central role in the entire health care system (as, of course, they had been doing all along). In medical centers throughout the country, growing interest in ‘health maintenance’ and its accompanying insurance designs seemed poised to catapult PCPs from the role of nerds to quarterbacks. Then, for reasons we don’t have the space to discuss here, in the following years in many settings, the quarterbacks got recast as gatekeepers, and then as switchboard operators. Delivering primary medical care remained as innately vital and sacred a job as ever, but the stature and daily work of the PCP (with the second P now standing for ‘provider’) became degraded in many settings. Morale sank, and PCP burnout and dropout became more common. What does all this have to do with academic detailing? A lot. One of the most frequent and visible ways that the quarterback-to-gatekeeper degradation has developed is in the role of clinical decision-making – for medications most often, but also about test ordering, specialist consultations, and many other choices the primary care clinician faces daily. In the Olden Times, which still survive in some pockets of our pathologically heterogeneous coverage system, these decisions are still left in the hands of the PCP, and are still made well or poorly by individuals. But increasingly, such choices are driven by formularies, prior authorization requirements, algorithms, and other restrictions. Sometimes these are thoughtful, evidence-based guidances that are useful antidotes to the occasional wild and crazy choices some practitioners occasionally make – ‘freedom’ which can on occasion lead to potential harm to both patients and health care budgets. But sometimes the restrictions are simple-minded, financially-driven, and disrespectful of the needs of specific patients and the nuanced judgment of the individual clinician. That’s where academic detailing comes in. There will always be a place for formulary limitations and restriction of the worst non-evidence-based decisionmaking. But wouldn’t we all rather live in a medical world in which decisions are primarily shaped by the informed decisions of a well-trained health care professional, updated through discussion of the latest data? Especially if that information was provided by another savvy clinician equipped to have a back-and-forth conversation about the basis and the pros and cons of trial findings, guidelines, and observational research? That would help primary care clinicians make better decisions without all the limitations of arbitrary insurance requirements, or computer-based algorithms that sometimes function as if they know Mrs. Johnson better than her doctor does. It could also pave the way for wider adoption of the evidence-based recommendations that the more enlightened policies seek to achieve. And clinicians could again feel more like the health care professionals we spent so many years learning how to be. Join us for Dr. Avorn's annual conference talk at #NaRCAD2016: Innovations in Clinical Outreach Education.  Biography.
Jerry Avorn, MD | NaRCAD Co-Director Dr. Avorn is Professor of Medicine at Harvard Medical School and Chief of the Division of Pharmacoepidemiology and Pharmacoeconomics (DoPE) at Brigham & Women's Hospital. A general internist, geriatrician, and drug epidemiologist, he pioneered the concept of academic detailing and is recognized internationally as a leading expert on this topic and on optimal medication use, particularly in the elderly. Read more.
0 Comments
NaRCAD's Interview Series: Public Health Detailing Program at New York City Department of Health and Mental Hygiene (DOHMH) Featuring Michelle Dresser, MPH, Senior Manager, Programming & Strategy Tags: Detailing Visits, Diabetes, Evaluation, Obesity, Program Management, Smoking Cessation, Training  Thanks for taking the time to share the great clinical outreach education work that’s being done by the NYC Department of Health and Mental Hygiene, Michelle! Tell us a bit about yourself and how you got involved in public health, specifically public health detailing. Michelle: Thank you for the opportunity to speak about the Public Health Detailing Program. I have over 20 years of public health experience in both the non-profit and government setting, with the last 12 here at the New York City DOHMH. Throughout my professional career, my specialty has been in healthcare marketing and provider education, emphasizing how providers and consumers can better communicate with each other by tailoring complex messages using health literacy principles.
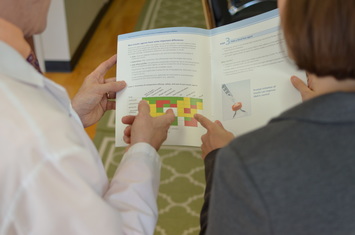
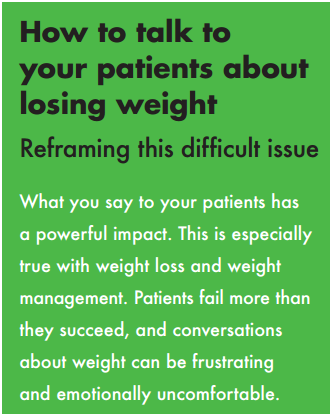 An excerpt from DOHMH's obesity pocket guide. An excerpt from DOHMH's obesity pocket guide. It’s essential our reps have excellent selling and communications skills, so when they engage providers and get their buy-in, providers are then equipped to get their patients “on board”. One-on-one provider engagement helps them understand how important it is to have a 2-way communication with patients. How can an outreach representative encourage providers to “get on board” and think about care as a dialogue? Michelle: Let’s use obesity as an example. With obesity, both providers and patients are frustrated, for different reasons. Providers may be frustrated that patients’ comorbid conditions are being exacerbated or don’t have the same kinds of tools to treat obesity as they do other conditions; patients might feel that providers aren’t using great communication techniques, like motivational interviewing (MI), to help them set goals and take small steps towards the goal. If a patient is only told, “You need to lose weight,” which is such a broad and overarching goal, they’ll be frustrated, and frankly, non-adherent. I know I would be. 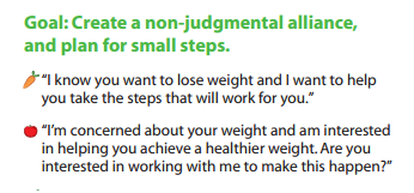 Example of a coaching script created by DOHMH. Click to learn more. Example of a coaching script created by DOHMH. Click to learn more. Encouraging providers to have specific dialogues using a customized approach for each patient is important. This kind of dialogue takes into account patients’ literacy beyond the written and spoken word—it looks at scientific, fundamental, health and cultural literacy, too. We work on “coaching scripts”, which take the key recommendations and reframes them in order to custom-tailor the conversation for each patient.
One thing that’s unique about public health detailing is that we detail the whole team through one-on-one interactions. Evidence shows these types of interactions with providers and staff are more effective at changing behavior; however, sometimes due to the makeup of the practice we must conduct group presentations. It’s not ideal, but it still allows us to get the messages and materials out there.
 A coaching guide designed by the NYC DOHMH to aid clinicians in smoking cessation support for patients. A coaching guide designed by the NYC DOHMH to aid clinicians in smoking cessation support for patients. So when an outreach representative goes into an office, they detail...everyone? Michelle: If there are 15 people who work in an office, we’re going to detail all 15 of them. It’s a lot! Sometimes, the person who is the champion of a new behavior or workflow isn’t going to be the provider. We see the front desk staff as instrumental; they’re interacting with all of the patients. We work with our teams to ensure even the front desk staff receives the materials and information, rather than seeing them merely as a “gatekeeper” to get to the providers. Sounds like a lot of training goes into preparing for your campaigns, and for thinking about the entire process of effective outreach. Tell us more about your trainings, and about how you prepare outreach representatives on disease content training, as well as in marketing and communications skills.  Click to view more Public Health Action Kits (copyright of NYC's DOHMH) Click to view more Public Health Action Kits (copyright of NYC's DOHMH) Michelle: On average, our trainings are about 5 days in length and take place the week prior to launching a new campaign. About 40 percent of the training is disease content, so we work with our internal Health Department experts, as well as external experts, where we learn about prevention strategies, treatment strategies, epidemiology and the landscape around the key recommendations chosen based on the evidence of that topic. We need to know the ‘why’ behind the campaign. Once we have that under our belt, we shift to sessions on how to frame the issue, how to promote the materials, figuring out the “features and benefits” as well as the “barriers and objections” and finally “gaining a commitment”, which are phrases that come from pharmaceutical marketing. We’re “selling” and promoting public health interactions, so we work on those skills. We also do a great deal of role playing, including videotaped analysis of each rep. We look at body language, what communication skills are effective, we do knowledge assessments, quizzes—we make sure our team is well-prepared to go out and detail. We take this seriously—they’re representing the New York Department of Health and Mental Hygiene.
What’s a major barrier your program has faced, and how have you tackled it? Michelle: A big challenge, when starting a detailing program, is access. The landscape of healthcare systems in NYC has drastically changed over the past few years. As an example, several years ago, the majority of our Brooklyn territory was almost entirely made of up of small practices where access wasn’t an issue. What’s changed since then? Michelle: Now, many of these sites have become part of larger institutions, so there’s corporate buy-in that needs to happen for people to come in and talk to the staff. As I mentioned before, although we try and limit group presentations, this has proven to be an effective strategy when entering into a new relationship. Once they get to know us and recognize the value of the program, they’re engaged in having us come back to conduct 1:1 visits on the follow-up and subsequent campaigns. How do you know when a campaign is working and becoming successful? Michelle: Evaluation is always on the top of our priorities, and can be a challenge for any program to evaluate effectiveness. For every campaign we conduct an initial and follow-up visit where we assess provider practice. This allows us to see if there has been a change in practice from the initial to the follow-up visit. Additionally, we rate what providers intend to adopt in terms of the key recommendations and supporting tools and resources. We also collect a large amount of qualitative data because it's also critical to gaining a more complete picture of the campaign’s success, especially when reporting on barriers, access and materials.
You can scale this up or down, depending on your need and organizational priorities. Our program focuses on where there’s the greatest need and potential for greatest impact. Programs should make sure to look at their organization’s agenda and goals. It’s important to look at the data and plan the best course of action within the capacity you have. Biography: Michelle Dresser. Michelle Dresser is the Senior Manager of Programming and Strategy for the Public Health Detailing Program within the Bureau of Chronic Disease Prevention and Tobacco Control at the New York City Department of Health and Mental Hygiene. In this role, she oversees the overall programmatic direction and strategy of the program. This includes, campaign strategy and timing, campaign content, training and economic incentive development, provider selection, identification of targets to ensure the greatest impact on populations most in need, and identification of “new needs” opportunities to expand program reach and achievement of program goals. She also oversees internal and external strategic relationships to enhance programmatic objectives.
The exponential increase in computing power and data storage capacity, coupled with the sharp decrease in data processing costs, have made possible an era of ‘big data’ that is transforming many aspects of life and commerce. In health care, this evolution is enabling access to information that was impossible to imagine in the era when I first began this work when most prescriptions and test orders were still written on little scraps of paper. As applied to academic detailing, this growing capacity opens up a veritable armory of double-edged swords. Knowing what doctors are ordering: This information has always been an important advantage of the pharmaceutical industry, which routinely buys the detailed prescribing records of specific physicians from intermediaries such as IMS, who in turn purchase these records from nearly every pharmacy in the nation. In the hands of an agile pharmaceutical representative, knowing a doctor’s drug preferences can be a powerful tool in shaping a promotional message tailored to that person.
 Many of us in have had mixed views about the use of such data. On the one hand, it can make possible a more precisely focused discussion about optimal ordering of tests and treatments that is based on a given practitioner’s actual behavior. On the other hand, the approach comes with several risks. One is the concern that clinicians may feel “spied upon” – a problem that doesn’t seem to come up much in industry visits. This in turn can divert the conversation to discussion of “Why are you visiting me?” rather than a conversation about optimal patient care. Data feedback to clinicians also degenerates frequently into he said-she said debates that often come down to “My patients are different!” We welcome feedback from academic detailing programs on how this use of data has worked (or hasn’t) in their own settings. What patients are (or aren’t) doing: The computerization of dispensing records opened an era of hitherto-difficult research on patient adherence to their medication regimens, with generally depressing findings of low adherence. The full import of this rampant epidemic of non-compliance is still not well understood by most prescribers. The rapid growth in mobile and wearable technologies that capture physical activity and other lifestyle choices provides another potential source of data on patient behavior, but the best applications of this information are even less well understood. In principle, academic detailing programs embedded in health care organizations can provide feedback to clinicians on how much or how little their patients are taking medications as directed or complying with other medical advice, and – more important – what to do about it. Is this a useful component of the educational encounter? Again, we would welcome hearing how this use of big data to provide feedback on adherence or patient behavior does or doesn’t fit into the work of ongoing academic detailing programs.
In the coming years, we will see even greater access to terabytes of data on who is ordering what, and what patients are doing with their prescriptions and other treatments. Used well, this technological revolution can provide added power to programs designed to improve that clinical decision making. Expert Trainer Insight Series, Part 2:An Interview with Amanda Kennedy, PharmD, BCPS, Director of the Vermont Academic Detailing Program Tags: Detailing Visits, Expert Training Insight Series, Rural AD Programs, Training  Dr. Amanda Kennedy & NaRCAD's Dr. Jerry Avorn Dr. Amanda Kennedy & NaRCAD's Dr. Jerry Avorn NaRCAD: Hi, Amanda! We’re looking forward to chatting with you. You’ve been an academic detailer for about 13 or 14 years—tell us about the Vermont program. Amanda: The Vermont Academic Detailing Program was started in 1999, by Amy Jaeger, PharmD. I trained with Dr. Jaeger as a pharmacy resident. When she left Vermont in the early 2000s, she wanted to leave the program to someone who would be passionate about evidence-based prescribing in primary care. So the job was mine! Amy unfortunately passed away unexpectedly in 2005, but her mentoring and passion for patient care has stayed with me, and has forever shaped the way I think about pharmacy and academic detailing. We’ve evolved over time into a more organized program, with a grassroots focus of serving our state’s primary care providers. This commitment to service is how we succeed in building strong relationships with providers over time, and we infuse the spirit of service into all of our sessions.  NaRCAD: What challenges do you face that are specific to being a rural program? Amanda: Our program has been stable, but it's been low budget over time. Despite being a small state, we face many challenges balancing the feasibility of delivering sessions to providers with our rural geography. The evidence-base for academic detailing clearly demonstrates the value of a 1:1 ratio of academic detailer to provider. However, it doesn’t make sense for us to travel 2 hours each way to see one provider only to repeat the process the next day for a second provider within the same practice. So we mostly deliver small group academic detailing sessions, as a way to serve as many providers as possible within our budget. We‘re mindful that “small group” means about 3 prescribers, which matches the types of practices we serve. NaRCAD: Along with being a seasoned academic detailer, you also help us here at NaRCAD to train groups of new detailers at our Boston-based techniques trainings. Can you share some highlights? Amanda: The power of the NaRCAD trainings is in the power of the individuals who attend. Realizing that other people are struggling with the same issues, and trying to address these issues with academic detailing, is so powerful.
 Amanda works 1:1 with a trainee at a 2016 NaRCAD course. Amanda works 1:1 with a trainee at a 2016 NaRCAD course. NaRCAD: What would you tell someone who’s thinking about coming to a future NaRCAD training? Amanda: I'd tell them to have fun with it! This training is a special opportunity to focus on how to best communicate with people around behavior change. It allows one to put aside specific topics and come together in a group to think about how best to deliver complex information. The model applies across topics, allowing people from all types of programs to work towards a common goal. The training is hard work, but so rewarding, and offers the chance to learn and network with other trainees. The best part is that it’s immediately applicable upon returning to your program. NaRCAD: That’s good advice—we agree that learning opportunities should be both challenging and enjoyable. In other news, we heard you recently presented at a U.S. House of Representatives Congressional Briefing. Tell us about that. Amanda: I was invited to present at the briefing entitled, “Getting the Medications Right”: An essential ingredient in achieving the goals of H.R. 4878 – the Medicare Better Care, Lower Cost Act. The briefing was presented by the American College of Clinical Pharmacy and the College of Psychiatric and Neurologic Pharmacists. The purpose of the briefing was to highlight pharmacists as members of the primary care team. I specifically presented some of my Vermont research that involved partnering pharmacists within patient-centered medical homes. It was the perfect opportunity to showcase the innovative work we are doing here in Vermont. I think there was a great response from those who attended and for me personally, it was an absolute honor to be there.
NaRCAD: Thanks so much for taking the time to connect with us, Amanda. We’re delighted to have you as part of our core team of training facilitators, and we’re excited to share what you’re doing in Vermont with our community. Learn more about Amanda Kennedy, or visit our Team Page to learn more about NaRCAD staff. Join Us: NaRCAD's next training is open for registration.
Ask the Expert: Questions for Amanda? Ideas for us? Thoughts on detailing? Share your response in the comment section below for community discussion!  Director Dr. Mike Fischer chats with trainees about their goals. Director Dr. Mike Fischer chats with trainees about their goals. Bevin K. Shagoury, Communications & Education Director @ NaRCAD Tags: Detailing Visits, Training We’ve just wrapped up our Spring Academic Detailing Training here in Boston, and we're excited to share a recap of an important event. With each new class of trainees, we see new ways that academic detailing can improve health outcomes for a variety of topics and populations. This May 16th & 17th, the NaRCAD team hosted 18 trainees from across the U.S. and Europe. Our trainees represented programs looking to increase STD screening and sex education in Philadelphia, reduce overmedication of elderly long-term care residents across Indiana, teach safer opiate prescribing in Wisconsin, and implement other quality improvement initiatives in Ireland, Denmark, Georgia, Rhode Island, and North Dakota.
 Join us at our next training event. Join us at our next training event. Everyone at NaRCAD would like to thank our fantastic, enthusiastic class of trainees for participating. We’ll be keeping in close touch as they go out into the field to implement important academic detailing interventions. For other members of our community, we hope you’ll consider joining us this Fall at our next 2-day course on September 19th & 20th, 2016--it's the core of what we do. If it helps to convince you, 100% of our trainees from this week's course said they'd recommend our course to a colleague, so save the date, and be sure to register early as space is limited and seats fill quickly. Registration opens on June 15th-we're looking forward to seeing you there! Until then, remember: "Good information doesn't disseminate itself."  Tags: Autism, CME, Conference, Detailing Visits, Pediatrics, Practice Facilitation, Training NaRCAD: Hi, Meagan and Mindy—thanks for taking the time to talk with us about your clinical outreach education programming at Colorado ABCD. Can you give us an overview about ABCD and its mission to improve child development? Meagan Shallcross: Colorado Assuring Better Child Health & Development (ABCD) works with community partners, pediatric healthcare providers, early learning providers, and families across Colorado communities. The goal is to strengthen systems and identify children with developmental delays, connecting them with community services as early as possible.
 Meagan Shallcross, MPH Meagan Shallcross, MPH NaRCAD: Tell us a bit about your backgrounds. How did you each get into healthcare improvement? Meagan: My background in public health, along with experience working in clinical settings and behavioral science research, developed my interest in healthcare improvement that aims to bridge community work and clinical practice, standardize clinical workflows, and ultimately improve experiences and outcomes for patients and families  Mindy Craig, PA-C, M.S. Mindy Craig, PA-C, M.S. Mindy Craig: My path to healthcare improvement is a little different than what you might expect. I worked for Northwest Airlines as a flight attendant for several years straight out of college. At that time the airline industry was losing a large amount of money and needed to find a new way of operating. They decided to utilize a Total Quality Management approach and enlisted people from every department to undergo training in TQM and then facilitate small departmental groups in quality efforts. It was through this process that I began to understand the importance of doing business with a quality framework.  Learn more at coloradoabcd.org. Learn more at coloradoabcd.org. Eventually, I left Northwest and started working in a Neurology clinic while going back to school with the goal of becoming a PA. After completing my degree I worked in primary care settings for about 10 years. I participated in small clinic QI efforts over the years and continued to be interested in quality improvement. I was hired by ABCD 8 years ago to bring a clinical perspective to their physician outreach. It was a natural progression for me to start approaching our work at ABCD with a quality improvement framework. The power of engaging front line staff to implement changes that result in improvement remains as strong as it was when I worked in the airline industry. NaRCAD: Talk with us about your academic detailing programming at ABCD—you’ve been doing this for about 10 years, right? Mindy: We started our work encouraging the use of standardized developmental screening tools in the primary care settings. This was supported by the American Academy of Pediatrics policy statement in 2006 recommending the use of these tools at well child visits. We offered informal outreach to physicians providing instructions on screening tools, billing information, AAP recommendations and information on referral resources. We quickly recognized that screening alone wasn’t sufficient and began talking about the referral process and how to ensure successful referrals were being made. At around this time, research was showing us that only about 50% of children referred for Early Intervention services were actually connecting to that referral. It was easy to identify children with concerns but not as easy to ensure they received needed support. We decided to try formalizing our approach to outreach by offering Continuing Medical Education [CME] credits. While we didn’t change content, offering CME changed the way providers saw us as detailers. We appreciated the new credibility, but still struggled with recruiting new practices. NaRCAD: Recruiting practices to participate is a challenge for many programs. How did this struggle transform into quality improvement?
We now offer Quality Improvement [QI] and MOC projects for implementing developmental screening, autism screening and postpartum depression screening in addition to a project that aims to increase the percentage of children who successfully connect with Early Intervention when referred from their primary care provider. We have been thrilled with the response from physicians for participating in these projects and just received funding to continue and grow our outreach efforts. NaRCAD: What have been some other challenges you’ve faced when going in to talk to clinicians about implementing developmental screening? Mindy: I started working at ABCD unsure of how to provide physician outreach, so I naturally modeled my efforts on the one successful approach I knew very well, which was pharmaceutical sales. As the recipient of pharmaceutical detailing, it was pretty easy to begin my outreach efforts in a similar fashion. I quickly learned how it feels to be a detailer. Front office staff rejected me repeatedly, I made hundreds of phone calls that didn’t get returned, and when I did get to speak to a provider I had to speak quickly and to the point to keep their attention. The challenge of gaining access was the biggest barrier I confronted early on and remains at the top of the list.
 A key challenge: gaining access to clinicians. A key challenge: gaining access to clinicians. NaRCAD: When dealing with those challenges, what’s helped you to build relationships with clinicians in order to gain commitment? Meagan: To deal with the challenges that arise, we have found that it helps to get creative in our approach to gain access to clinicians and add credibility to our messages. A barrier we have encountered when trying to schedule times to meet with clinicians is the expectation that we will provide food. Our funders and budgets do not allow us to pay for food, so we have opted to provide other incentives for clinicians, such as CME or MOC credit. Not only is offering CME/MOC credits an educational incentive for providers, but it lends credibility to our messages. We facilitate our QI projects through multiple meetings at the practice and have found that, by developing relationships and a presence in the office, we can overcome clinicians’ resistance to implementing screening or other changes in their practice.
 Resource and best practices exchange at #NaRCAD2015 Resource and best practices exchange at #NaRCAD2015 NaRCAD: We were happy to see you at our 3rd International Conference on Academic Detailing here in Boston a few months ago. Tell us more about how the conference helped you think about your work in a different way. Mindy: We were thrilled to be able to attend the conference and came away very energized. We highly recommend the conference to anyone doing similar work. Some of our key “take-aways” were around the fundamentals of academic detailing, including the need for profession materials and repeated visits to develop relationships. We came home committed to find money for developing professional materials and to attend the two-day intensive training offered by NaRCAD.
However, I’ve struggled with our role as a non-profit in meeting these needs. Up to this point, ABCD has utilized a very hands-on approach. We plan meetings, take notes, write up PDSA cycles, make “To Do” lists – anything we can do to make the process easy for the practice and allow the providers to concentrate on patient care. A true practice facilitation model is more concerned with increasing the capacity of the practice to continue quality improvement work after the facilitation had ended. The goal isn’t to do all the work, but to help the practice find capacity to do it themselves. NaRCAD: What other advice would give to a new and emerging AD program that’s just getting started, or that you’d give yourself if you could go back in time 10 years? Meagan: We have found NaRCAD’s training and tips to be very helpful, so we would recommend that new clinical educators attend a NaRCAD techniques training to hone their skills in communicating their messages with clinicians and gaining commitment to behavior change. One of our main takeaways from the NaRCAD conference was the importance of high-quality, professional materials, so we would recommend that new programs budget for the development of professional materials as well as food, which can be an incentive when setting up meetings with clinicians. Over the years, we’ve realized how critical it is to work with community partners before going into healthcare practices to ensure that clinical workflows, such as processes for making referrals to external agencies, are aligned with community-defined processes and so that clinicians are aware of the resources available to patients and families in their communities. NaRCAD: Thanks so much for sharing important insights from your program to improve childhood health outcomes. We look forward to seeing you at a future training and hearing more about your program's future successes! BiographiesMindy Craig, PA-C, M.S., Director of Physician Outreach, has been with the ABCD team for 8 years and brings with her experience in the clinical setting. She earned her physician assistant degree at the University of Colorado Health Science Center’s Child Health Associate/Physician Assistant program in May 2000. Concurrently, she completed additional course work and research to earn her Master of Science degree in Pediatrics. Ms. Craig worked as a physician assistant in a number of settings for ten years prior to joining the ABCD team. Her medical career has included a variety of medical office positions from medical records clerk to practice manager. This range of experience positions her to fully understand the unique dynamics and flow in a typical office, which allows her to deliver technical assistance to practices at a meaningful level.
Ms. Craig’s quality improvement experience began in the business sector where she was extensively trained on Total Quality Management (TQM) at Northwest Airlines. She worked at the airline as a facilitator, training inflight and ground personnel in the principles of quality improvement. This experience with quality continued in the clinical setting, as she has participated in and/or chaired a number of quality improvement projects over her career as a physician assistant. In addition to her work at ABCD, Ms. Craig also does consulting work for organizations needing assistance with physician outreach and education. Meagan Shallcross, MPH, Healthy Steps/Physician Outreach Coordinator, joined the ABCD team in June 2015 as the Healthy Steps and Physician Outreach Coordinator. Meagan is passionate about building systems and environments that support children’s healthy development through clinical-community partnerships and integrated care delivery approaches. Meagan earned a Master of Public Health degree at the University of Michigan, where she supported Patient and Family Centered Care projects at the university health system and was involved with community-based participatory research addressing health equity, as well as research focused on provider-patient communication. Learn more at www.coloradoabcd.org. All photos used with permission.  Trainee Update Series: Where Are They Now? Bevin K. Shagoury, Communications & Education Director Tags: Cancer, Detailing Visits, Practice Facilitation, Training Hi, Emily! We’re happy to reconnect with a NaRCAD trainee, and to feature your current work on this month’s blog. Can you tell us a little about yourself and how you ended up working at the National Colorectal Cancer Roundtable? I’ve worked in public health for 12 years, and in seven of those years I’ve focused on cancer screening and prevention. I got to know NaRCAD while working at the Washington State Department of Health, where I designed their approach and curriculum to coach primary care clinics and health systems on quality improvement strategies to increase colorectal cancer screening. Then last summer I joined the American Cancer Society as the National Colorectal Cancer Roundtable’s new associate director. In this role much of my work is still focused on developing educational resources for providers, but I’m also involved in efforts to increase colorectal cancer screening through other channels, such as public education and policy. I learned so much about effective methods for conducting clinical education from the NaRCAD Academic Detailing training that I participated in back in October 2012. I’m grateful to have the opportunity to reconnect with NaRCAD, and thank you for the opportunity to share an update on my work! Tell us a little bit about background and goals of the Roundtable. The Roundtable, established by the American Cancer Society (ACS) and the Centers for Disease Control and Prevention (CDC) in 1997, is a national coalition dedicated to reducing the incidence of and mortality from colorectal cancer in the U.S., through coordinated leadership, strategic planning, and advocacy. Today, the Roundtable is a collaborative partnership with more than 100 member organizations across the nation. Through the efforts of several task groups, the Roundtable advances initiatives that focus on provider education, public education, health policy, quality and disparities issues. Thanks in part to the work of many of our members, colorectal cancer incidence and mortality rates have dropped by over 30% in the U.S. among adults 50 and older in the last fifteen years, with a substantial fraction of these declines due to screening. Yet, despite the good news, colorectal cancer remains the second-leading cause of cancer death in the U.S. when men and women are combined.  The Roundtable is focusing on a great initiative called “80% by 2018.” What’s the story behind this movement? To accelerate efforts to increase colorectal cancer screening, the Roundtable launched the 80% by 2018 initiative in March of 2014. 80% by 2018 is a movement in which hundreds of organizations have committed to substantially reducing colorectal cancer as a major public health problem and are working toward the shared goal of reaching 80% of adults aged 50 and older screened for colorectal cancer by 2018. To date over 650 organizations – including medical professional societies, academic centers, survivor groups, government agencies, cancer coalitions, cancer centers, payers and many others – have signed a pledge to make this goal a priority. If we can achieve 80% by 2018, 277,000 cases and 203,000 colorectal cancer deaths would be prevented by 2030. You can learn more about 80% by 2018 and pledge your organization’s support on our 80% by 2018 webpage.  A trainee role-plays at a NaRCAD 2-day techniques session. A trainee role-plays at a NaRCAD 2-day techniques session. You attended a NaRCAD Academic Detailing Training a few years back to practice skills in clinical outreach education. Can you tell us a little bit about the highlights of your experience? Academic detailing and practice facilitation are relatively new fields, so when I first accepted a job that included these skills I felt a little in over my head! I was up for the challenge, though, since I saw provider education and training as a way to move further upstream in making substantive and sustainable changes that would positively affect public health. It can take a while for new clinical findings to get implemented in primary care, so I saw that academic detailers and practice facilitators serve a key role in getting these findings into clinical practice. My two-day Academic Detailing Training with NaRCAD taught me practical skills to work in this role, and gave me the confidence to know I could be effective without a clinical background. The highlight was the role-playing and one-on-one feedback from experienced academic detailers. Their personal feedback was not something I could have found in a book or online training. What tools from the training do you think are most relevant to active detailers in the field? Some of the most valuable tools I took from the training were the interpersonal skills needed to be effective as an academic detailer. The tips on how to solicit buy in after sharing a practice change was incredibly useful, such as asking: “does this sound like something you’d be willing to try in your practice?” It was also really helpful to learn how to approach sharing a clinical update that could potentially make a provider feel as though they had been delivering inappropriate care. The training taught me how to navigate these discussions by saying that while something might be common practice it’s no longer supported by the latest clinical evidence. In my experience, providers were very receptive to learning new clinical updates when it was shared in such a way that they did not feel they were being reprimanded for not knowing already knowing the latest evidence. Thanks for chatting with us. We’re happy to help get the word out about “80% by 2018” and looking forward to hearing the results of the initiative. Thank you for the opportunity! I enjoyed reconnecting with you and reflecting on how my training with NaRCAD has enriched my work in clinical education. I’d like to encourage any readers that are interested in 80% by 2018 and efforts to increase colorectal cancer screening to learn about the campaign. And there are lots of great tools and resources in the provider education section of our website that might be of particular interest to academic detailers.  Emily Butler Bell is the Associate Director of the National Colorectal Cancer Roundtable. In this role she manages a number of projects that support the 80% by 2018 initiative, a movement in which hundreds of organizations are working toward the shared goal of reaching 80% of adults aged 50 and older screened for colorectal cancer by 2018. Prior to joining the Roundtable, Emily served as the Cancer Screening Quality Improvement Consultant for the Washington State Department of Health, where she designed their approach and curriculum to coach primary care clinics and health systems on quality improvement strategies to increase colorectal cancer screening.
Prior to that, Emily worked with the American Cancer Society in Austin, TX as a Cancer Information Specialist and later as a Health Insurance Specialist, where she gained insight into the access and affordability issues surrounding colorectal cancer screening. She holds a Master’s in Public Health from Boston University and a B.A. in Psychology from the University of California, Santa Cruz. Director's Letter We’ve just celebrated the 5th anniversary of NaRCAD, the only national resource center and network advancing clinical outreach education. We’re also celebrating a terrifically successful 2015. Highlights included running two sold-out academic detailing techniques trainings here in Boston; traveling to San Francisco and Oklahoma City for two customized off-site trainings; and bringing everyone together for #NaRCAD2015: Motivating Change, Transforming Care, our most successful annual conference so far.
We’re proud of it all, and more, including the brand-new NaRCAD Website—enjoy and explore a new gateway to academic detailing, including more interactive resources and expanded opportunities for connection, learning, and sharing. With so much to celebrate from 2015, we’re setting the bar high with big goals for the year ahead. Here’s what we’ll be up to in 2016, with you as our partners: Transformative Trainings: Registration for our May training in Boston is open and already filling up fast! We’re also happy to be in high demand for at least 5 “on-the-road” educational sessions and related projects across the US this year. If you want to learn more about the ways we can share our resources and expertise to help your clinical outreach education program grow and succeed, let us know—we’d love to learn about what you’re doing and see how we can help. #NaRCAD2016: Collaborating to Create Change. Our annual conference is the capstone of the year, so mark your calendars for November 14-15, 2016. What’s new this year? #NaRCAD2016 will feature opportunities to submit a proposal to showcase your clinical outreach education experience, data, and insights with the rest of the NaRCAD community. Keep your eyes on your e-mail and our conference page for more details about submission, coming soon. More Collaboration for Improved Health Outcomes: With 5 years of partnerships under our belt, we’re continuing to connect every day with new colleagues working in the field of AD and clinical outreach education. We’re excited to keep expanding our community and creating opportunities for deeper collaboration across programs. We invite you to stay connected as we continue to publish new blogs and interviews, feature partners on our network directory, expand our Learning Center offerings, and recommend evidence-based health news and events on our social media feeds. Most of all, our team wants to hear from you! Drop us a note to tell us what you’re doing, and tell us how we can help strengthen your program and highlight your successes. See you this year! Dr. Mike Fischer  Attendees share resources during a networking break. Attendees share resources during a networking break. Bevin K. Shagoury, NaRCAD Communications Tags: Conference, Detailing Visits, Jerry Avorn, Opioid Safety, Practice Facilitation The excitement and breadth of content in this November’s 3rd International Conference on Academic Detailing exceed what we can capture in this blog post. The combination of exciting speakers, engaging panelists, expert breakout session leaders, and national and international attendees eager to problem-solve created a forward-thinking event that inspired all of us working on AD and related outreach educational activities. As you reflect on our event's highlights, we encourage you to access on-demand video, speaker biographies, session descriptions, and more at our Conference Hub resource page.  Dr. Coffin of SFDPH and Dr. Fischer of NaRCAD Dr. Coffin of SFDPH and Dr. Fischer of NaRCAD Kicking Day 1 off and setting the tone for the entire event, NaRCAD Director Dr. Mike Fischer warmly welcomed our packed room at Harvard Medical School’s Martin Center by encouraging collaboration, connection, and sharing. Our Day 1 Keynote Speaker Dr. Carolyn Clancy, the CMO of the Veteran’s Health Administration, described the VHA’s work to improve pain management in the veteran population while addressing the challenges of medication abuse and overdose. Dr. Clancy shared strategy and data behind the national effort and the critical role of academic detailing in it, connecting attendees to a big-picture view that can be adopted to look at other health epidemics and interventions. Our first expert panel presented Practice Facilitation in Primary Care. Andy Ellner moderated the session, leading panelists Ann Lefebvre of North Carolina's AHEC Program, Lyndee Knox of LA Net, and Allyson Gottsman of HealthTeamWorks to discuss strategies, contextualize their work in relation to academic detailing and quality improvement, and share their personal approaches to challenges in primary care behavior change. Allyson Gottsman’s much-appreciated analogy that practice facilitation is not unlike “leading a fisherman to a well-stocked pond” resonated with panelists and participants alike. Many attendees who were actively engaged in practice facilitation in their daily work shared that the panel helped them to think about their work in a new way.  Breakout leaders share a moment during the Day 1 session! Breakout leaders share a moment during the Day 1 session! The afternoon’s breakout sessions offered attendees multiple tracks with AD-related topics to explore: deconstructing and analyzing a 1:1 AD visit, exploring the skills needed to manage an effective AD program, and strategizing on ways to identify and harness stakeholder support when initiating a new program or strengthening an existing one. The afternoon closed with two presentations; the first, by Terryn Naumann of the Canadian Academic Detailing Collaboration (CADC), offered participants a view of the power of synergy and teamwork, the historical context of the CADC’s creation and growth, and the future of the collaboration.  Dr. Avorn gives a presentation one Tweeter called "pure gold" Dr. Avorn gives a presentation one Tweeter called "pure gold" The final presentation of the day was a lively one by NaRCAD’s co-founder and co-director, Dr. Jerry Avorn, who identified major obstacles to effective evidence-based communication in the current landscape of healthcare, and provided a future-centered lens through which attendees could envision how academic detailers can address these challenges. A full day of new ideas and connections culminated in a networking reception that gave attendees a chance to relax and connect socially. Day 2’s morning opened with another engaging Keynote Speaker; Dr. Don Goldmann, CSO & CMO of the Institute for Healthcare Improvement, combined quality improvement theory with personal anecdotes, weaving in real-life examples of successful interventions to provide context and dimension to the theory that underlies all of our work.  L-R Valerie Royal, Joy Leotsakos, Sameer Awsare, Mike Fischer. L-R Valerie Royal, Joy Leotsakos, Sameer Awsare, Mike Fischer. More examples of successful practice change were illustrated by the morning’s Themed Plenary on the Intersection of Public Health and AD. Dr. Phillip Coffin of the San Francisco Department of Public Health shared the success of an intervention focusing on co-prescribing of naloxone to reverse opioid overdose deaths in San Francisco. Another successful AD intervention was presented by Michael Kharfen of the Washington D.C. Department of Health, who highlighted the successful implementation of AD programs to increase HIV and Hepatitis C screening and treatment. The afternoon featured our second Expert Panel, this time on the role of AD within integrated healthcare systems. Moderated by Dr. Mike Fischer of NaRCAD, panelists Joy Leotsakos of Atrius Health (MA), Sameer Awsare of Kaiser Permanente Medical Group (CA), and Valerie Royal of Greenville Health System (SC) shared their experiences using AD in systems at different stages of development. Attendees had the opportunity to discuss this topic further in the afternoon’s breakout sessions, which also included a session on practice facilitation, as well as third session to continue to explore AD and public health partnerships.  Happy to see our colleagues from Norway at #NaRCAD2015! Happy to see our colleagues from Norway at #NaRCAD2015! The conference’s closing discussion was led by Mike Fischer, who thanked not only the speakers, panelists, and session leaders, but the participants, whose willingness to share their experiences within an interactive setting was key in creating solutions to bring back to use in their daily work. The creative collaborations, exchange of resources, excitement in combating challenges in the field, and belief in the importance of AD for the future of healthcare transformation were felt by all at the closing of a very full and thought-provoking event. Our Twitter feed tracks the event’s highlights through #NaRCAD2015, and you can catch our event photo album on our Facebook page. We invite you to explore these topics, learn about our speakers and attendees, and connect with us at the NaRCAD Conference Hub, where you can access on-demand video of all main sessions from the conference. Thank you again to all who attended, and to AHRQ for funding our series. Please stay in touch with us and each other, and continue the conversation and idea sharing below. We hope to see you in 2016!  Jerry Avorn, MD, NaRCAD Co-Director
Tags: Detailing Visits, Jerry Avorn, Training Often, in discussing academic detailing programs with current or potential sponsors, the question comes up: “Wouldn’t it be cheaper just to deliver the message to a whole group of clinicians at once, instead of the much more cumbersome process of talking to prescribers one at a time?” Sure, it would be cheaper. So would just mailing (or e-mailing) memos to people telling them what to do, or requiring time-consuming groveling on 1-800-DROP-DEAD prior authorization numbers before a costly resource can be ordered. The problem is that cheaper solutions often don’t work, or don’t work well. We have decades of proof that putting health care professionals together in a darkened auditorium and subjecting them to a PowerPoint Tolerance Test does not reliably change behavior. The main reason that academic detailing relies on one-on-one interactive communication is that it is the best way for the outreach educator to accomplish several key goals:
Well-trained academic detailers understand this, and they use the interactivity to craft a real-time, care-improvement message that best addresses the learning needs (and attitudes and biases!) of the person they’re visiting. Less competent academic detailers force their “targets” to sit still while they administer a canned micro-lecture monologue, which works poorly. They may feel they “got through all the points” they wanted to cover, but if there was no interactivity, no conversation, then the person they were talking at might as well have been falling asleep in a darkened amphitheatre. We know this is the case from decades of experience and scores of randomized controlled trials. We also know, perhaps most compellingly, that when the drug industry wants to change what we know and about its products, it sends people to our offices to talk with us—it doesn’t rely only on the less expensive modalities of mailings, e-messages, and sponsored lectures. So the next time someone suggests that it might be more inexpensive to just gather prescribers into a big room and have someone talk at them for an hour, agree with them. Then point out that it’s also less time-intensive to scarf down a Big Mac than eat a real meal, shoot off a series of emoticons rather than a personalized note, or listen to a ring tone of a Beethoven sonata rather than hear it performed by musicians. Cheaper isn’t everything.  Mike Fischer, MD, MS, NaRCAD Director
Tags: Conference, Detailing Visits, Director's Letter, Opioid Safety NaRCAD is thriving, thanks to the engagement and enthusiasm of our network of healthcare professionals working to improve patient outcomes. The best way to become more involved in that network is to join us for our 3rd International Conference on Academic Detailing. This year’s conference will be our most exciting and interactive event to date, with a stimulating 2-day program bringing together thought leaders for expert panels, best practices, breakout tracks, networking, and invigorating group discussions on innovations in the field. Our keynote presentations will provide critical insights for everyone working to improve healthcare quality and patient outcomes. On Monday, Nov. 9th, Dr. Carolyn Clancy, Chief Medical Officer of the Veterans Health Administration, will highlight the VA’s use of academic detailing to address the epidemic of opioid overdose and misuse to save veteran’s lives. On Tuesday, Nov. 10th, Dr. Don Goldmann, Chief Medical and Scientific Officer at the Institute for Healthcare Improvement, will provide his insights on how to engage front-line clinicians in committing to change – drawing on IHI’s years of experience in promoting patient safety. Many questions about academic detailing still need to be explored, new ideas generated, and connections made. We need to foster solution-based discussion from a wide range of voices, representing clinical education, public health, practice transformation, government, the non-profit sector, hospital networks, academic institutions, and others. But the most important ingredient for the success of this event is you. Join us as we work together to discover solutions, connect you with others that can amplify your impact and elevate your work, and share your experiences and insights on the best ways to navigate a rapidly-changing healthcare landscape. We hope you’ll join us this November 9th and 10th, and that you’ll help us spread the news about this unique, transformative event. See you in November!  Behind the Scenes with Dr. Doyle-Tadduni, NaRCAD Training Facilitator
Editor’s note: In this series, DETAILS asks Academic Detailing (AD) Techniques Training facilitators how they lead by example, challenge participants, and ensure that trainees are ready to go out into the field. Dr. Doyle-Tadduni focused on her insights and tips to success in providing excellent clinical education by building strong detailer-to-clinician relationships based on evidence, clarity, and “intrinsic trust.” Tags: Cardiovascular Health, Detailing Visits, Expert Trainer Insight Series, Training NaRCAD: Hi, Mary Liz! We’re looking forward to learning more from you about what it’s like to train prospective academic detailers. But first, tell us a little about how you became involved in detailing. Dr. Doyle-Tadduni: I began working as an academic detailer about 10 years ago in Pennsylvania with the Independent Drug Information Service, which is sponsored by PACE (Pharmaceutical Assistance Contract for the Elderly). My clinical background in nursing and my teaching background within various university settings has served me well in this role as a clinical educator. NaRCAD: What does a day of academic detailing look like for you? What successes and challenges do you see? Dr. Doyle-Tadduni: My territory encompasses the westerns suburbs of Philadelphia where I visit physicians, nurse practitioners, and physician assistants. I see these providers in a variety of settings, including private practices, university-affiliated practices, and outpatient health care systems. Since AD is a new concept to many practitioners, it’s essential to start your visit by educating providers about the importance of academic detailing and how it will benefit them and their patients. In this way, I’ve developed many long-standing relationships with providers who have said that AD has been very beneficial for their individual practices. It’s very gratifying in a follow-up appointment to hear that a provider has taken the evidence you provided and put it into practice, creating a positive outcome for patients. NaRCAD: How do you build strong relationships with the clinicians you visit? Dr. Doyle-Tadduni: There needs to be an intrinsic sense of trust between a detailer and the provider. You may not gain the trust in the relationship during your initial visits, but when you provide clinicians with a full understanding of the importance of your visit, along with presenting educational materials that are credible and evidence-based, you promote trust and strengthen the relationship and gain clinician commitment to changing behavior for the better. NaRCAD: You’ve facilitated quite a few trainings with us at NaRCAD. Tell us more about the course, and why you enjoy doing it. Dr. Doyle-Tadduni: This course is a great support for both new and seasoned trainees in enhancing their detailing skills, as well as program managers who oversee a clinical education program and need a greater understanding of how best to run an effective program. At the beginning of the training, the trainees absorb AD theoretical content and techniques, and on Day 2, they’re actively practicing the techniques and role playing different educational encounters in small groups. The program trainees have been wonderful people to meet! I’ve had the opportunity to meet people from all over the United States, and some from Australia, Portugal, and Europe. It’s been very interesting being involved with the trainings and hearing about health care in other regions of the US and abroad. Despite the miles that separate all of us in our different demographics, we all have similar challenges in our respective health care systems. NaRCAD: As a trainer, you “play” the role of the clinicians during breakout group sessions, presenting different personalities as well as various behavioral and content-based objections to the material or the visit. Tell us more about this part of the course. Mary Liz practices with a trainee, teaching the importance of showcasing AD as a service that will create better outcomes for clinicians’ practices and patients. Dr. Doyle-Tadduni: We present the trainees with many different role play scenarios where they can actively practice overcoming obstacles that get in the way of earning clinician commitment. Finding the right delivery of your messaging can be very challenging, depending on the environment, and every detailer will have a unique set of potential obstacles to face at each visit. The key is to focus on the evidence, so that practitioners can realize how beneficial it will be to their practice. The training’s small group role play practice sessions provides trainees ample opportunity to practice, ask questions, perfect their skills, and be prepared to face inevitable obstacles in their own future visits. NaRCAD: What do NaRCAD trainees need to have to be ready to succeed as a detailer? How does our 2-day training help to get them ready for success? Dr. Doyle-Tadduni: The trainees need to have an expert knowledge base of the clinical topic and related materials they’ll be presenting during a visit. They also need to present AD as an on-going resource. With busy practitioners being so tightly scheduled through the day, programs designed to assist them in improving how their practice runs is a plus. By the end of the two days of training, the trainees will have a strong foundation of clinical education techniques, and they’ll be forming ideas about implementing these efforts in their respective programs. NaRCAD: Any closing thoughts or advice for new trainees, or first time detailers as they prepare to head into the field? As long as you’re well-versed on the material you’re delivering, and you’re presenting yourself as an “ambassador of the evidence”, you’ll have the tools you need to ensure that an academic detailing visit is truly successful.  An Interview with Frank Leone on Treating Tobacco Dependence with AD
Dr. Leone directs Penn’s Comprehensive Smoking Treatment Program and was a former trainee with NaRCAD. Tags: Detailing Visits, Smoking Cessation, Substance Use, Training NaRCAD: Tell us a bit about yourself. How did you get into academic detailing? Frank Leone: I’m a pulmonologist, and have been focused on the treatment of tobacco dependence for over 20 years. In my early years, I had always been amazed at how infrequently my colleagues would approach the literature for solutions when facing this common problem in the clinic. It seemed to me that they relied heavily on “common sense” approaches and techniques derived from misunderstandings, rather than consulting published guidelines and available standards. I became interested in the behavioral economics of tobacco treatment decision-making in the clinic, and realized that traditional approaches to changing physician behavior might be inadequate for dealing with a cultural problem this well-entrenched. We initially turned to NaRCAD for advice on Academic Detailing in 2011, and found the approach to have just the right potential to both meet the needs of the target audience, and allow us to deliver our message in a cost-effective and scalable way. We were also given an opportunity to work with the Philadelphia Department of Public Health as they started up their efforts to influence the local provider culture around tobacco, and we’ve been “off to the races” working within our community, creating positive changes, ever since. NaRCAD: What does your program focus on? (What health issue does it address, and what clinician behavior are you seeking to change?) Dr. Leone: Our Academic Detailing (AD) program focuses exclusively on tobacco dependence treatment. As you can imagine, that problem cuts across a number of different audiences. Our detailers work with physicians, psychologists, nurses, counselors and others to impact the rate at which tobacco treatment services are delivered in our area. We use AD to address the limits in knowledge base around pharmacotherapy, as well as to shape the core assumptions about effectiveness of treatment in key patient populations (e.g. those with established lung disease or serious mental illness). NaRCAD: Tell us about some of the growth you’ve seen and been a part of as it relates your program. Dr. Leone: Our AD program has grown every year since its inception. We started out focused on primary care physicians in underserved parts of Philadelphia. From there, we expanded our target audience to include specialist physicians, nurses, and nurse practitioners. Most recently, our audience has expanded to include behavioral health practitioners in both inpatient and outpatient settings. Because of our success using AD to work with care providers from a variety of disciplines, we are currently exploring ways to extend AD principles to “system-wide” approaches to creating behavior change. NaRCAD: What would you say are the greatest challenges you see in implementing this intervention? Dr. Leone: Finding the right people to go into the field is imperative. Over the years, I’ve been impressed that success during the AD interaction is less about what degree a person has, and more about the ability to be gently directive, while willing to truly listen. Detailers need to be spontaneous and responsive to their audience, while at the same time keeping their inner eye on the target. This is a skill that takes a little time and training to develop. It sounds like it ought to be an easy thing to do, but we’ve found that an organized, logical, mentored approach to learning these skills is important to success. NaRCAD: How about what works well? How do you know when you’ve been successful? Dr. Leone: We always try to incorporate some sort of measurement tool into our AD projects. It might be about knowledge, attitudes, or behaviors, but having a metric to gauge our impact is important feedback ensuring we stay on mark. Our funders appreciate a concrete measure of change as well. If I could figure out how to capture this, my favorite measure would measure the “A-ha!” moments that happen so often within the audience. I love the look of epiphany in the clinician’s eye when a detailer has found a way to make the information relevant and transformative. That’s when I know we’re really making change for the long run. NaRCAD: You attended our Academic Detailing Techniques Training a few years back. What are the most useful resources or information that you’re still using today? Dr. Leone: Truthfully, the greatest resource has been the continuing relationship with the NaRCAD team. On multiple occasions during the conception and start-up phases of our project, we were able to touch base with professionals who had a large collective experience in diverse disciplines to get some great tips and suggestions. On one specific occasion, I remember sharing a written detailing piece with the NaRCAD team. We had developed it in hopes of getting some feedback. Not only did we get great advice, but it was professional advice – complete with references, examples, resources, and connections to the theoretical basis for the suggestions. To me, this is the kind of interaction that helps my team grow and learn over time. NaRCAD: What does future success look like for you? Dr. Leone: In twenty years, when you go visit your doctor for your annual check-up, and you hear him or her say, “Of course tobacco dependence is a chronic illness of the brain for which there are a number of effective treatments. It’s hard to believe we used to simply tell people to stop!” –then you’ll know we’ve done our job well. Biography: Dr. Leone received his medical degree from the University of Pittsburgh, School of Medicine, and completed his postgraduate training in both general internal medicine and pulmonary / critical care medicine at Thomas Jefferson University Hospital. He also received his masters degree in clinical epidemiology and biostatistics from the University of Pennsylvania School of Medicine. Dr. Leone directs Penn’s Comprehensive Smoking Treatment Program, a clinical program of the Penn Lung Center, located at both Penn Presbyterian Medical Center, and the Perelman Center for Advanced Medicine. The new program provides state-of-the-art and individualized treatment to smokers, including those with co-morbidities. Dr. Leone’s scholarship focuses on investigating advanced treatment strategies for tobacco use disorder, and on testing educational strategies for improving the care of the tobacco dependant patient. Dr. Leone is a member of several professional and scientific societies, including the Society for Research on Nicotine and Tobacco, the American College of Chest Physicians, and the American Thoracic Society. He has served the Commonwealth of Pennsylvania as a legislative appointee to the Governor’s Tobacco Use Prevention and Cessation Advisory Committee since 2001. Dr. Leone has been invited to speak at numerous lectures on topics of smoking treatment and pulmonary medicine, and has been published in a variety of clinical and research journals. He is board certified in pulmonary and critical care medicine. Learn more and review related publications on the University of Pennsylvania’s site. Read more: Behavioral Economic Insights into Physician Tobacco Treatment Decision-Making : Leone, Frank  Mike Fischer, MD, MS
Tags: Cardiovascular Health, Detailing Visits, Smoking Cessation, Training At NaRCAD, we work together with our many partners, collaborating on important interventions to improve patient health through clinical outreach education. This summer, we’re especially looking forward to a unique collaboration to improve cardiovascular health, as we travel to Oklahoma to support the Healthy Hearts for Oklahoma project, part of AHRQ’s EvidenceNow initiative. EvidenceNow is a group of 7 large studies across the United States working to improve cardiovascular care in small primary care practices. Along with materials development and program support, the NaRCAD team will travel to Oklahoma City in July to train over 20 health professionals, teaching them how to provide the service of academic detailing to participating practices. Focusing on the ‘ABCS’ (aspirin use, blood pressure control, cholesterol management, and smoking cessation), the professionals we train will carry out academic detailing visits in order to present best evidence to participating practices. By using the skills and techniques of AD to assess the needs of clinicians and practices throughout Oklahoma, the detailers we train will gain commitment from clinicians to commit to practice change. The Healthy Hearts for Oklahoma project will visit hundreds of practices, tracking these practices’ behaviors over time. Ultimately, the evidence generated by Healthy Hearts and the other EvidenceNow studies will yield key insights about how best to bring evidence to diverse practice settings and improve the cardiovascular health of all Americans. Supporting organizations that are carrying out important work such as this is at the core of who we are and what we do. The positive impact of academic detailing can be amplified with each new intervention, program, or even a single visit to a clinician. As we enter into our 5th year as the only nationally available resource center for for academic detailing, the strength of the relationships we build makes it possible for clinical outreach education to serve more practices and have a greater impact on patient health. We’ll share highlights from the Healthy Hearts for Oklahoma project and other exciting collaborations with our subscribers this fall. In the meantime, we’d love to see you at a future Boston-based training, or at our 3rd annual International Conference on Academic Detailing this fall—join us as we work together to advance the field of clinical outreach education. Jerry Avorn, MD, NaRCAD Co-Director
Tags: Detailing Visits, Health Policy, Jerry Avorn, Medications For over a century, appropriate medication use in the U.S. has relied heavily on the regulation of what manufacturers can say about their products. One of the first powers given to the Food and Drug Administration when it was created in 1906 was the ability to require that makers of “patent medicines” state what was actually in their products. (Often, it was a mixture of ineffective ingredients laced with alcohol or opium, but accurate information was a start.) Over time, the agency was granted the authority to regulate claims about efficacy and safety that companies made about prescription drugs. This has begun to change, with potentially important implications for academic detailing. Currently drug manufacturers promoting their medications to clinicians are limited to discussing indications for which they have obtained approval from FDA, Last year, however, FDA announced its openness to considering policies to make it easier for drug manufacturers to present doctors with their own views about off-label uses of their products that FDA did not consider appropriate. A follow-up “draft guidance” would similarly open the door for manufacturers to provide information about side effects that differs from the determinations of FDA scientists and outside advisers. Most recently, the agency has revealed plans for a national conference on whether limiting drug-makers’ promotional statements might infringe on these companies’ corporate free speech rights. And a bill that has progressed through Congress, The 21st Century Cures Act, will make it easier for drugs to be approved on the basis of looser standards, including lab tests or other surrogate measures of efficacy rather than actual patient outcomes. These developments will have important implications for academic detailing. If we are entering a period of lessened government regulation of what pharmaceutical manufacturers are permitted to tell prescribers about off-label uses of their products, or their safety profiles, there will be an even greater need for balanced, evidence-based communication to inform medication use decisions. Just as travelers to developing countries that have polluted water supplies often prefer to drink bottled water, clinicians may increasingly feel the need for access to non-contaminated information sources if they can’t be sure what’s coming out of an increasingly de-regulated informational tap. All of us concerned with optimal use of medications will need to monitor these developments closely. If the proposed changes prevent FDA from regulating the promotional claims made by drug manufacturers as closely as in the past, then health care systems and individual practitioners will have increasingly greater need for the more reliable sources of information that academic detailing services can provide. Stay tuned.  An Interview with Paula Walker, Clinical Pharmacist
Baylor, Scott & White Health | Dallas, Texas Tags: Cardiovascular Health, Chronic Illness, Detailing Visits, Elderly Care, Training Tell us a bit about yourself. How did you get into care redesign and transitional care? I grew up in the area of Inman Square Pharmacy in Cambridge, Massachusetts. After graduating from Northeastern University in 1990, I began my career in community pharmacy. Soon after I entered the pharmaceutical industry, I spent many years representing the biological division of Rhone-Poulenc. I continued to keep connected with public health by practicing in the community part time; I’ve also been serving in a family practice clinic for over 8 years now. Three years ago, upon recommendation from our clinic director, I joined The Institute of Chronic Disease and Care Redesign at Baylor Scott and White Health in Dallas. Tell us about the institute. What does your team focus on with regards to providing transitional care? What approach do you take? Our multidisciplinary team focuses on improving outcomes among chronically ill older adults. Our innovative approach includes using advanced technology to identify patients at most risk for readmission. With a focus on heart failure, COPD, and pneumonia, patients are identified and supported as they transition from one level of care to the next. Our transitional care team encourages each specialty to work at the very top of their license to assist patients whose recovery is complicated by cognitive impairment, frailty, and social issues. Our team shares offices together so each discipline is available to all team members at all times. A strong team and constant communication is the key to our success. What does a typical day or week look like for you in this field? How do you incorporate academic detailing techniques into your work? My role is to perform the medication reconciliation on all of my patients and communicate any concerns with the appropriate providers. I attend weekly rounding with my team and need to be able to make and support any medication recommendations. In terms of using academic detailing techniques, our team practices evidence-based medicine in the care and treatment of our population with chronic disease. It’s also key for a pharmacist in this role to be able to communicate to providers quickly and effectively regarding drug selection, dosage, and titration. Learning and practicing the skills required to communicate effectively in this environment is essential. In a typical day I will consult with a geriatric specialist, cardiology, nephrology, APRN, social worker, and corporate administration. That is a lot of communicating! You attended our Academic Detailing Techniques Training a few years back. What parts of the program worked well for you, and what are the most useful resources or information that you’re still using today? I found the skills learned during the NaRCAD training to be useful and confidence building. There is an art to being able to research information then applying it to support a recommendation in a short amount of time. NaRCAD brings together professionals from different disciplines that are focused on improving the communication of science-based information in their practice or facility. It is useful to connect with others that require these skills in their work. The small class size made it very easy to meet all the participants and learn from their experiences. I believe you can never be too experienced, and I constantly learn from the experience of others. What are some future successes you’re looking forward to in your work and in the field in general? As we prepare to expand the Transitional Care Model at Baylor Scott and White Health under the population health infrastructure, I look forward to the pharmacist’s role to expand as well. Our goal of disease management, well above the national standard, will require evidence based medicine and the sharing of clinical information to all members of the care team. I look forward to continuing my relationship with NaRCAD—together we can help each other transform care, resulting in an improvement in the quality of life for our patients. And I’m looking forward to NaRCAD’s 3rd International Conference on Academic Detailing this November in Boston! Biography: Paula Walker, Clinical Pharmacist, joined the Baylor Scott & White Health Transitional Care Team in 2012. Paula is the team pharmacist and oversees all medication reconciliation for their older adult population with heart failure, COPD, and pneumonia. Prior to joining BSW, Paula has worked in community pharmacy, clinic pharmacy (still active), and the pharmaceutical industry. Paula holds BS in Pharmacy from Northeastern University.  by Lyndee Knox, PhD Tags: Detailing Visits, Practice Facilitation, Primary Care Practice facilitation is an approach to helping primary care practices improve the quality of care they deliver to patients. Good practice facilitation is practice-centered, meaning that you start where you’re needed and work out from there. One of my favorite stories about the practice-centered nature of facilitation was told to me by Ann LeFebvre, director of the statewide primary care facilitation program in North Carolina. Ann was starting work with a new practice in her community. As is common at the beginning of most improvement efforts, she asked the practice what their greatest concern was at the moment. Ann expected them to tell her they were concerned about improving workflow with their electronic health records, or that they wanted to improve their performance on particular HEDIS (Healthcare Effectiveness Data and Information Set) measures, or that they wanted help engaging their patients more effectively. Instead, what they told her caught her completely by surprise. “We’re really concerned about our patients getting to our practice.” “Oh,” she said, “so you’re worried about access issues?” “Well, sort of,” the staff person responded. “Recently we’ve had a flock of geese take up residence in our parking lot, and they are biting our patients when they get out of their cars to walk inside. Some of our patients are afraid to get out of their cars.” 5 Whys Tool: Click to Learn. As an experienced facilitator, Ann understood how important it was to meet practices where they are at the current moment, not where they “should be.” So she rolled-up her sleeves and said, “Ok, let’s figure this one out.” She saw the problem of the geese as an opportunity to teach practice staff basic principles of quality improvement. She taught them to use the “5 Whys” to determine why the geese were in the parking lot in the first place, and then to use Plan-Do–Study-Act cycles (PDSA) to design and test solutions to the “goose attack” problem. Working together, Ann and the practice discovered that a woman living next door to the practice used to keep and feed the geese. She had recently been hospitalized and because she was no longer there to feed them, the geese had moved into the practice parking lot. Staff developed a solution: to have another neighbor feed the geese – and tested this solution using a PDSA cycle. The geese left the parking lot, their patients no longer had to deal with hungry and aggressive geese in the practice parking lot, and staff had started to build capacity in quality improvement! Practice facilitators are specially trained individuals who work with primary care practices “to make meaningful changes and develop the skills they need to adopt new clinical evidence and health service models in their work and to sustain these changes over time.” (Knox & Brach, 2011; DeWalt, et al., 2010). The primary aim of facilitators, whether working alone or as part of team, is to build practice capacity for continuous quality improvement, as well as to strengthen practice ability to adapt and implement new evidence-based treatments and health service models. Facilitation teams develop long-term relationships with practices. They may work with a practice intensively for 6 to 10 months to implement a specific improvement and then step back for a while. Even though the active facilitation project has ended, they will check-in with the practice every month or two to monitor progress and maintain relationships until they are needed to support another significant improvement project at the practice. While facilitation can be provided by a single individual, (a “practice facilitator”) it is often a “team sport.” The facilitation team is usually led by an individual with expertise in quality improvement processes and methods. This person serves as the team leader and primary point of contact with the practice, and brings in his or her team mates to help the practice as needed. Other members of the facilitation team include individuals with expertise with health IT who can help practices optimize their health IT systems to support the desired changes; team members with expertise in setting up data systems for monitoring performance; and most recently, patient partners. Academic detailers are also essential members of most facilitation teams. They possess deep knowledge about clinical topics and provide 1:1 education to clinicians to increase their knowledge about specific preventive care and treatment issues, encouraging those clinicians to change their behavior to improve patient health. A number of excellent resources are available for training members of facilitation teams, and to guide development of a practice facilitation program. These include the PF Handbook, the National PF Curriculum, and the How to Start and Run a PF Program. Dr. Mike Fischer, the director of NaRCAD, and a team of experts in PF and practice improvement helped develop them. These and other resources that can assist you in building a practice facilitation program in your area can be accessed here. Lyndee Knox, PhD is founding director of LA Net, a primary care practice based research and resource network established with funding from the Agency for Healthcare Research and Quality (AHRQ) in 2002. LA Net supports research and innovation in the healthcare safety net in Los Angeles and provides practice facilitators to practices in its network to support practice-based, clinician and community-led research, evidence translation and practice improvement. Dr. Knox served as principal investigator on AHRQ’s Task Order 13 (TO 13) to examine the use of practice facilitators to implement the Care Model in the safety net, and convened the AHRQ Practice Facilitator Consensus Panel to summarize the state of the field as part of TO13. Most recently she led work for AHRQ to produce a manual to support formation of new practice facilitation programs across the U.S. The resulting manual, Developing and Running a Primary Care Practice Facilitation Program: A How to Guide and case studies are available on AHRQ’s website. As director of LA Net, Lyndee has served as lead on a 2 year contract with the Greater Los Angeles Veterans Administration to create and train a cadre of internal coaches to support its primary care teamlets and PACT transformation. Currently she is working with Mathematica Policy Research to create a 30 module training curriculum for new Practice Facilitators/Coaches for the U.S. AHRQ. Dr. Knox also directs Project ECHO LA, a replication of the successful quality improvement and clinical education intervention from the University of New Mexico aimed at increasing access to specialty care services in rural and underserved areas. Project ECHO LA has been supporting ECHO Knowledge Networks for the LA safety net for 3 years in areas including: psychiatry, preventive care, geriatric medicine and quality improvement.  Bevin K. Shagoury, Communications & Education Director
Tags: Detailing Visits, Training Our most recent 2-day Academic Detailing Techniques Training was held here in Boston on May 4th and 5th, 2015, and it was a successful and exciting convening of 18 trainees from all over the country. Clinical pharmacists, nurses, and program specialists gathered in Boston’s downtown to learn and practice social marketing techniques to use when educating front line clinicians about new evidence and important interventions. Our trainees will take these valuable skills back to a wide range of programs, with goals including improving health for veterans with PTSD, increasing referrals to smoking cessation programs, and strengthening chronic disease lifestyle management programs. Many of us have attended trainings and conferences heavy on Powerpoint presentations and light on practicing tangible skills. At NaRCAD, we use a dynamic curriculum wherein we integrate role-play, interactive large and small-group discussion, live demonstrations of a successful academic detailing visit, reflection through videography, ongoing networking, and the chance to learn from experts, clinicians, and colleagues through practice and skills sharing. After their training sessions are done, trainees move forward to establish new academic detailing programs, strengthen and develop existing ones, or use our techniques in other clinical education settings. And as their work continues, so does ours—we maintain contact with our trainees, providing critical resources and featuring their work on our website and DETAILS blog. This fall, we’ll be featuring partner profiles of many of our trainees’ academic detailing programs, so that our community can learn about the critical role these programs play in improving health outcomes. Join us at our next training this September—a program one recent trainee describes as “an excellent program, with fabulous faculty, and a well-run, valuable service to the healthcare community.” We keep improving our curriculum to ensure that each of our trainees gets personalized support to make their work easier. Their appreciation and feedback helps us to refine our training, encouraging us to think about ways we can continue to provide the best resources available. As the field continues to grow, so do we—and our trainees tell us that we’re making an impact by leveraging their work, sharing best practices, and running “the best training I’ve ever been to—seriously!”  Spring 2015 Director’s Letter
Mike Fischer, MD, MS, Director of NaRCAD Tags: Detailing Visits, Director's Letter, Training Despite the difficult winter weather in Boston, NaRCAD has been off to a great start so far this year. We’ve been very excited to begin several new initiatives with terrific partners. As we move forward through 2015 and beyond, we invite those of you reading our newsletter and following us through our blog or on social media to reach out about working together on similar efforts. Training academic detailers is a core part of our mission, and we continue to have full registrations for our Boston-based training sessions, telling us that there’s an interest and a demand for our training course. This year we were thrilled to take our training on the road for the first time, working with the San Francisco Department of Public Health on several new initiatives, focusing on diverse topics including overdose prevention, increasing use of vaccinations in pregnancy, and HIV screening and treatment. This July, we’ll again deliver training outside of Boston, this time in Oklahoma to help support a new AHRQ-funded project aimed at improving care for cardiovascular risk factors in primary care. We also created and launched a new workshop for the experienced group of academic detailers at Atrius Health here in Boston. Similarly to our 2-day techniques training, we used role play and interactive group discussion to help clinical pharmacists work on overcoming barriers and obstacles. Interacting with Atrius’s dedicated group of outreach educators has all of us thinking about how academic detailers can best maintain and develop their skills over time, and we’re interested in hearing about how existing programs approach this challenge. If you have similar experiences to share, let us know—we’re always eager to share best practices with our network community of detailers, programs, and supporters. We want to hear from you. Your ideas matter–tell us how you’d like to collaborate, create new opportunities for academic detailing, and improve quality of care and patient outcomes.  by Joy Leotsakos, PharmD
Tags: Cardiovascular Health, Detailing Visits, Evaluation, Program Management, Training Who We Are. The Academic Detailing Service (ADS) of the Atrius Health Clinical Pharmacy Program provides clinically appropriate, evidence-based, cost-effective medication management in a multidisciplinary team setting. Our Clinical Pharmacy Program includes 15 clinical pharmacists (CPs) serving nineteen Internal Medicine and Family Medicine (IM/FM) ambulatory care practice locations. In the past four years, our program has evolved and transformed through evaluating our impact, absorbing and implementing internal feedback, and collaborating with others in the field, including NaRCAD. Our Start. As the program manager of our ADS, I’ve seen our service grow and change. When we began our program in 2011, it was as an administrative mandate to meet with all IM/FM prescribers once per fiscal quarter to deliver messages about cost-effective prescribing and clinical quality. We started by formulating a menu of topics to cover in our ADS work each quarter, including individual clinician prescribing reports reflecting performance on prescribing initiatives from the Pharmacy & Therapeutics Committee, specific questions to survey clinicians on a clinical topic, targeted education for low performers on prescribing initiatives, and various other ‘hot topic’ clinical issues. CPs detailed individual clinicians via formal 1:1 scheduled appointments, and also did so less formally (such as by catching them in the hallways) or in larger groups during department meetings. Is it Working? We documented our ADS activities by checking off the individual clinicians we detailed each quarter. At that time, there was no formal training for our CPs on how to conduct a detailing meeting. Unfortunately, this method of creating content for visits soon resulted in a large menu of topics so varied that each quarter’s detailing became unwieldy and too broadly focused. And our documentation, while it gave us a general sense of the number of clinicians detailed, did not tell us anything about the quality of this detailing. Room for Improvement. Our group is fortunate in that our ADS activities have always been accepted and even expected by our IM/FM clinicians. We experienced almost no clinician resistance to our educational meetings. But in 2013, when attending one of NaRCAD’s 2-day Academic Detailing Training sessions, I learned that we could make changes to improve our services, as well as my own skills as a detailer. As a result, we altered the format of our ADS program, choosing to detail clinicians in a 1-1 or small group format of less than 4. We also selected a goal of 90% of clinicians receiving detailing at least once every quarter. Evaluating Impact. We began evaluating the impact of the changes we’d made to our ADS, specifically choosing to look at its impact on a discretely measurable topic: reducing the unnecessary ordering of an ALT test (alanine transaminase) in patients on the ’statin’ cholesterol-lowering medications. We were able to demonstrate that our detailing of all IM/FM clinicians led to significant reductions in ALT ordering and meaningful cost avoidance for our organization. Asking for Feedback. With NaRCAD’s support, we further refined our program in 2014 based upon feedback from an internal focus group. By soliciting honest feedback from the CPs about their detailing experiences, I discovered considerable variation in how they approached the menu of topics provided each quarter and came to understand that the continuous process of visiting with each clinician at their sites often felt stale and repetitive. New Approach, New Results. We revised our ADS workflow to tie each round of clinician appointments directly to a specific and single P&T prescribing initiative. Furthermore, we developed a method to tag low performing clinicians for an ‘intense’ ADS visit and higher performers for a ‘touch’ ADS visit. We began this new workflow with an initiative to improve the use of evidence-based beta-blockers in patients with heart failure, a quality measure for the Medicare Pioneer Accountable Care Organization (ACO) project. Using this new approach, clinical pharmacists were able to deliver a fresh and meaningful message to the right prescribers, resulting in a change from 73.6% to 97.8%prescribing of evidence-based beta-blockers in this patient population. Partnering with NaRCAD for Ongoing Learning. In March 2015, we coordinated with NaRCAD again, and they provided our group of clinical pharmacists with a 2.5 hour workshop to enhance our AD skills. I’d encourage anyone who does this type of educational outreach to make use of this invaluable resource. Of course, our Atrius Health Academic Detailing Service will continue to grow and change as we find additional ways to improve our workflows and messages. I look forward to continued collaboration with NaRCAD and with others in the field, so that we can all keep learning from each other and improve health outcomes through effective academic detailing. Bio: Joy Leotsakos is a senior clinical pharmacist and the program manager for the Academic Detailing Service (ADS) of the Atrius Health Clinical Pharmacy Program. Joy joined Atrius Health in 2007 and became the program manager for the ADS program in 2012. Prior to joining Atrius Health, Joy worked as an assistant professor at Massachusetts College of Pharmacy and Health Sciences University in Boston, MA and provided ambulatory care pharmacy services to the South End Community Health Center also in Boston. Joy graduated with a Doctor of Pharmacy degree from Virginia Commonwealth University School of Pharmacy and then completed her residency in Ambulatory Care and Community Pharmacy at the University of Florida College of Pharmacy. Joy is the mother of one son, and enjoys salsa dancing, cycling and running in the summer and skiing in the winter. You can reach Joy by email at joy_leotsakos@atriushealth.org. |